Chapter 29
SYMPATHETIC OPHTHALMIA

SO is a rare, bilateral, diffuse granulomatous uveitis that presents insidiously after open globe injury or surgery. The injured eye is known as the exciting eye and the fellow eye, developing inflammation weeks to years later, as the sympathizing eye. Injury to one eye leading to damage in the other has been known since Hippocrates1 but was first well-described and termed SO only in the mid–1800s.2 Prior to steroid therapy, SO often led to a progressive, severe decline in vision.3
EPIDEMIOLOGY AND PREVENTION
SO is rare, but the true incidence is unknown because of a lack of pathologic proof, the difficulty in studying sufficiently large cases series,1 and the fact that most data are from the older literature, in which SO was often confused with other forms of uveitis.4 The incidence is:
• ~ 2/1000 following open globe injury;
• ~ 1/10,000 following routine ocular surgery5;
• decreasing with improved surgical technique6,7 :
 no SO in the Korean and Vietnam wars8;
no SO in the Korean and Vietnam wars8;
• equal between the sexesa;
• equal between the races, although
 higher pigmentation may increase inflammation and epithelioid cells9;
higher pigmentation may increase inflammation and epithelioid cells9;
• higher among the elderlyb;
• increasing with severe injuries;
• increasing with multiple ocular surgeries.
PEARL… Although SO may occur after closed eye surgery, it is most common with severe open globe injury/uveal prolapse. After the primary surgery, patients should be counseled about the possibility of SO and prophylactic enucleation (see Chapter 8).
CLINICAL PRESENTATION AND EVALUATION
Table 29–1 lists conditions in which SO has been reported.
• It has been seen as early as 5 days1 and as late as 60 years32,33 following trauma/surgery.c
• Approximately, two thirds of cases occur between 2 weeks and 3 months after injury3 and 90% are diagnosed within the first year.4
• Once SO develops, it can remain active for up to 30 years.34
| Any type of open globe injury1–4 |
| Perforated corneal ulcer10 |
| Any type of intraocular sugery11–21 |
| External beam radiation21 |
| Cyclocryotherapy22–24 |
| Laser cyclophotocoagulation25 |
| Radiation for choroidal melanoma21,26 |
| Contact/noncontact Nd:YAG cyclophotocoagulation27–31 |
Complaints in the fellow eye include:
• slight pain;
• sensitivity to light;
• accommodation problems; and
• mildly decreased visual acuity.
PEARL… Fellow eye complaints in patients with a history of trauma/surgery and bilateral panuveitis should always be taken seriously and require an urgent examination.
Early signs of SOd include:
• bilateral uveitis with AC cells/flare and a moderate to dense posterior vitritis35;
• ciliary injection;
• mutton-fat keratic precipitate on the corneal endothelium;
• thickened iris;
• iris nodules;
• synechiae;
• vitritis;
• optic nerve head swelling; and
• retinal edema, occasionally with serous retinal detachment and perivasculitis.35
In cases with prolonged inflammation, posterior synechiae and yellow nodules at the RPE (Dalen-Fuchs nodules) develop in the periphery. The diagnosis is more difficult when:
• the uveitis in the sympathizing eye is mild and nongranulomatous;
• the injured eye has been enucleated; or
• the patient is taking systemic anti-inflammatory medication.
Table 29–2 shows the conditions that have to be taken into consideration when the diagnosis is made.
FA shows multiple, deep pinpoint areas of hyper-fluorescence in the early arteriovenous phase, developing into larger areas of diffuse hyperfluorescence in later phases. The FA is nearly identical to that seen in VKH. The Dalen-Fuchs nodules display early hypo- or hyperfluorescence, followed by late leakage and staining.4,41,42
| VKH syndrome* |
| Phacoanaphylactic endophthalmitis |
| Sarcoidosis |
| Chronic idiopathic uveitis |
| Infectious granulomatous uveitis37,38 |
*Dysacusis, poliosis, vitiligo, alopecia, and lymphocytosis in the cerebrospinal fluid are common in VKH but rare in SO36; the diagnosis of SO, although usually made on the basis of clinical features alone, may be facilitated by the use of serum sialic acid and β2-microglobulin levels in dificult cases.39,40
PITFALL
Dalen-Fuchs nodules are present in less than 40% of eyes.
ICG acutely shows early hypocyanescence (which then subsides) and persistent hypocyanescence later.43
The long-term sequelae are highly variable:
• cataract (common);
• secondary (common);
• retinal and optic atrophy; and
• choroidal neovascularizatione (rare and may resolve spontaneously or with anti-inflammatory medication.
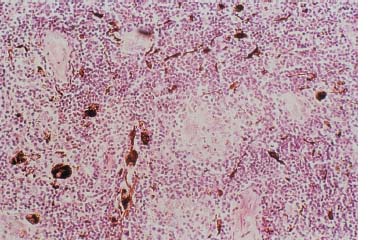
PATHOLOGIC FEATURES
Classic SO manifests as a diffuse, granulomatous choroidal inflammation with cellularf infiltration (Fig. 29–1).47 The original theory that SO is nonnecrotizing and spares the retina and choriocapillaris48 has been challenged.48,49 One pathologic review found retinal detachment in 58% and intraretinal inflammation in 42%3; another report showed focal choriocapillaris obliteration in 40%.48
PEARL… It appears that the retina, choriocapillaris, and optic nerve are initially spared but become involved late in the disease.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


