Suspension Microlaryngoscopy
In the event of laryngeal pathology that requires microscopic manipulation and removal (laryngeal papilloma, vocal cord nodules, vocal cord web, etc.), it is necessary to place a laryngoscope and stabilize its position to allow for the instrumentation. This frees both of the surgeon’s hands to accomplish the surgery.
33-1 Suspension Microlaryngoscopy
Operative Technique
1. The child is supine on the operating room table.
2. The otolaryngologist first examines the airway as described in the laryngology section, and then intubates the larynx with a laser safe metal tube (if laser use is anticipated) or with a regular endotracheal tube (if laser is not required), which is taped to the left side of the mouth.
3. A roll is placed beneath the shoulders to allow for complete extension of the head on the neck.
4. The table is placed in reverse Trendelenburg position to allow for comfortable viewing of the larynx through the operating microscope.
5. The laryngoscope is then reintroduced as described previously.
6. When the larynx is adequately visualized, the observer’s end of a self-retaining laryngoscope (Jako, Dedo, etc.) can be brought over to the midline so that minimal distortion of tissues is noted. A nonslotted laryngoscope should be used if a laser is to be used to avoid injury to local tissue, but a slotted laryngoscope may be used if a powered laryngeal shaver is used.
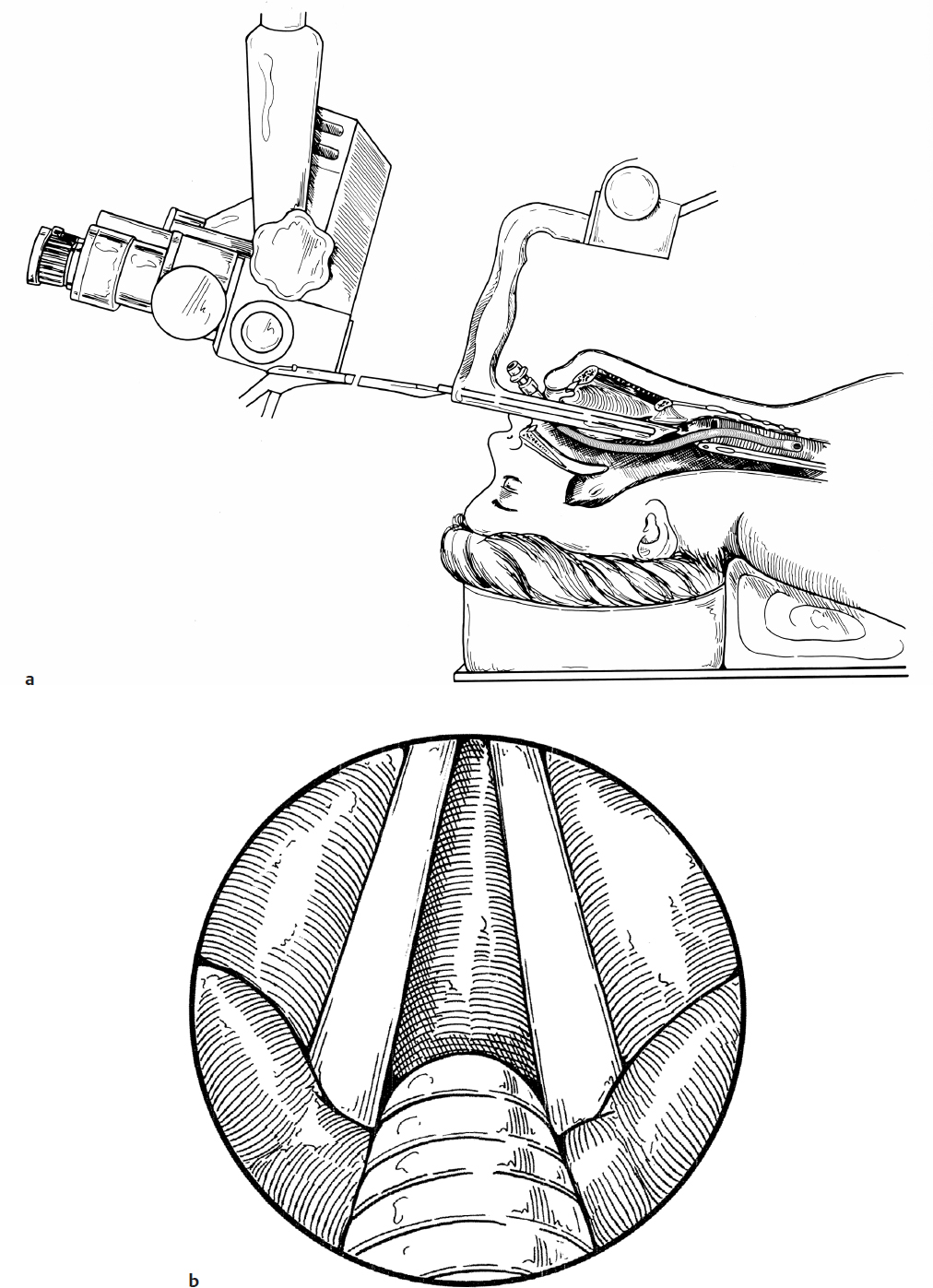
7. The laryngoscope is inserted deeply enough to view the entire anterior laryngeal structures (Fig. 33.1a).
8. The suspension apparatus is attached to the laryngoscope and then suspended from a Mayo stand or attached to the operating room table. This allows for movement of the entire table without disturbing the position of the laryngoscope.
9. The operating microscope is brought into place and the larynx is visualized utilizing a 400-mm lens (Fig. 33.1b). Instrumentation of the larynx can proceed with micro instruments and/or laser as indicated.
10. If a CO2 laser is used, the patient’s face must be covered with moist towels and the eyes with moist eye pads. No part of the patient’s face can be exposed. Operating room personnel must wear protective eye wear.
11. If examination of the posterior commissure area is required and this area is obscured by the endotracheal tube, the tube is removed and ventilation is continued using a Venturi Jet ventilation device. The Venturi device is placed through one of the light carrier channels of the laryngoscope and positioned above the laryngeal inlet. When adequately positioned, chest wall movement can be seen after each jet of air, and the laryngoscopy may continue without any obstruction in the larynx (Fig. 33.1c).
12. A rigid suction instrument placed through one of the light carrier channels can aid in continuous smoke evacuation during laser procedures. This is possible because illumination for this procedure is provided by the operating microscope.
13. At the termination of the procedure, the patient may be reintubated to recover from the anesthesia. This can be accomplished in one of two methods.
a. The laryngoscope can be removed and the patient intubated in a normal manner.
b. The child can be re-intubated even if a nonslotted laryngoscope is still in place.
1. The appropriate endotracheal tube (without the anesthesia adapter) is placed through the laryngoscope and into the laryngeal lumen (Fig. 33.1d).
2. The observer’s end of the tube is grasped with an alligator forceps and gently advanced as the laryngoscope is withdrawn (Fig. 33.1e).
3. The endotracheal tube is grasped at the level of the lips as it becomes visible as the laryngoscope is withdrawn.
4. The laryngeal forceps are removed.
5. The endotracheal tube adapter is placed on the end of the tube and adequate ventilation is resumed (Fig. 33.1f).
Complications
1. Laryngospasm
2. Glottic edema
3. Dental trauma