The non-functioning or dysfunctional sinus is completely isolated from the remainder of the nasal cavity with no hope of normal ventilation despite the most aggressive medical therapy. Most often these sinuses are the result of mucosal stripping/removal during prior radical surgeries. The reason for these radical operations include treatment of neoplasm, but most often is for revision of inflammatory disease when prior procedures have not been successful at restoring ventilation and maintaining patent ostia. When faced with a dysfunctional sinus, rhinologists typically have two choices: repeat the radical obliterative procedure or attempt to restore function and ventilation by reestablishing a drainage pathway into the nasal cavity. This latter option seems to represent the best long-term chance for surgical success in these difficult cases, with repeat ablative procedures as a last resort.
Frontal sinus
Dysfunctional frontal sinuses occur most often after failed frontal sinus obliteration (FSO), but can also occur after cranialization performed for inflammatory disease, trauma, or neurosurgical approaches. FSOs are known to have a failure rate of approximately 10%, and many times mucoceles occur years after the attempted obliteration. Although cranialization failure rates are not widely reported, they have been known to fail.
Considerations in the surgical approach for dysfunctional frontal sinuses include the patient’s original diagnosis; what substance, if any, was used to obliterate the sinus; and the anatomy of the frontal recess and surrounding skull base and orbit. If the situation permits, restoring ventilation to the sinus through reestablishing the natural frontal sinus outflow tract is desirable. With a neoplastic diagnosis, this technique will result in an aerated sinus that can be followed up endoscopically and radiographically for tumor recurrence.
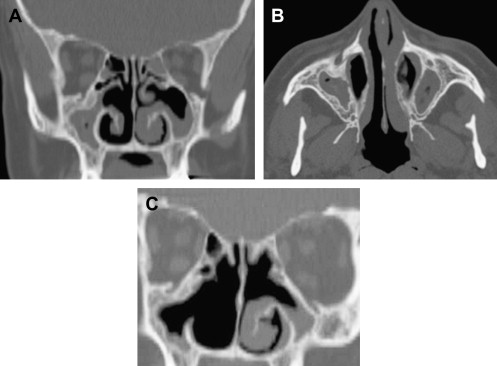
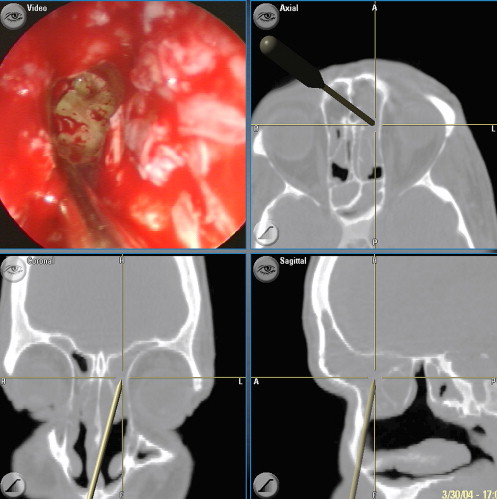
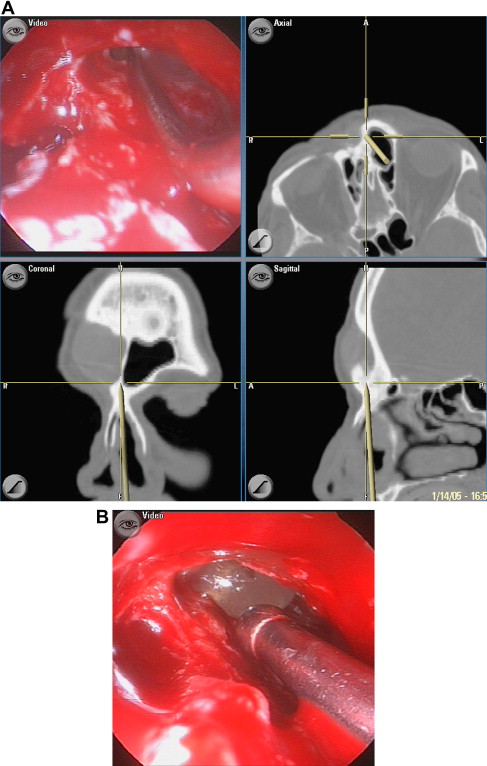
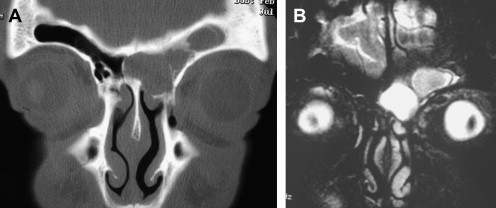
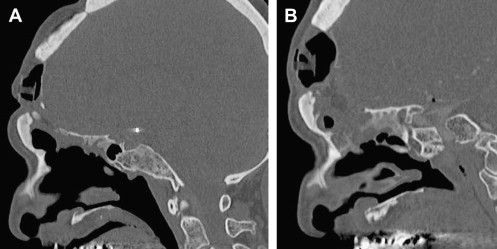
Obliterated cavities are particularly difficult to assess for recurrence, and this technique is generally not recommended when dealing with neoplasms. The substance used for obliteration also impacts the surgical approach. With fat obliteration, removal of all of the fat is typically not required, and simple restoration of the drainage pathway and removal of any grossly infected fat will result in success ( Fig. 1 ). Treatment of FSOs using hydroxyapatite or other alloplastic materials is typically much more difficult. These products often become infected and must be completely removed ( Figs. 2 and 3 ). Simple marsupialization of the sinus in these cases will not suffice.
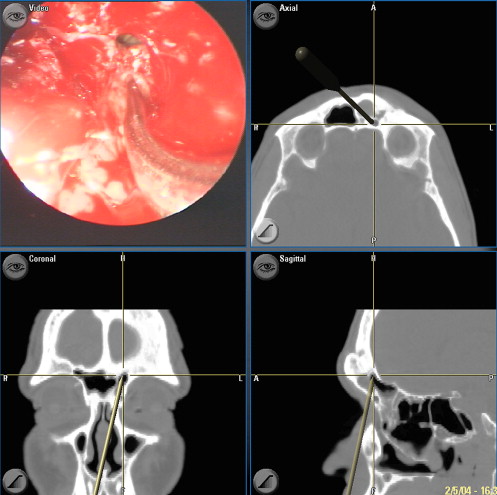
Finally, analyzing the anatomy adjacent to the dysfunctional frontal sinus is critical. Dehiscences into the anterior cranial fossa or orbit are very common. In these cases, removing every bit of mucosa from surrounding dura or periorbita to try to obliterate/ablate the sinus is even more difficult, and every effort should be made to restore some ventilation pathway into the nasal cavity. Mucoceles with anterior/posterior table dehiscences or orbital dehiscences do very well with simple endoscopic procedures. Additional consideration must be given to the specific location of the pathology, most often a loculated mucocele, on preoperative imaging when planning the surgical approach. Prior radical procedures that strip mucosa and even drill the bony confines of the frontal sinus often result in nonanatomic scarring and multiple loculated pockets ( Fig. 4 ). The precise location of these pockets can be difficult to access from below, and simple widening of the native frontal recess may not suffice.
The surgical algorithm to the dysfunctional frontal sinus is much like the approach to primary frontal sinus surgery ( Table 1 ). After taking into account the factors described earlier, the simplest approach, and one that is very often successful, is revision endoscopic frontal sinusotomy. Removal of residual agger nasi or frontal cells and any obstructing synechiae or lateralized middle turbinates often will open the frontal outflow tract (see Fig. 1 ).
| Procedure | Considerations |
|---|---|
| Endoscopic frontal sinusotomy | Marsupializes sinus, similar to revision endoscopic sinus surgery. |
| Endoscopic modified Lothrop | Most aggressive endoscopic marsupialization procedure. Needs advanced equipment and experience. |
| Inner sinus septectomy | Can be performed endoscopically or through a trephine. Results in a safe, ventilated sinus drained through a contralateral frontal recess. |
| Open approach for marsupialization and sinus preservation | Can be performed through existing scars/wrinkles, brow incision, or coronal incision. May be required for lateral pathology that is inaccessible from below. |
| Revision obliterative/ablative procedure | Requires major open approach to remove all mucosa from surrounding bone, dura, and periorbita. Significant long-term failure rate. |
In cases of severe osteoneogenesis caused by prior surgery or trauma, a simple frontal sinusotomy may not be possible ( Fig. 5 ), and an endoscopic modified Lothrop may be a reasonable alternative. Significant experience in endoscopic frontal sinus surgery and advanced equipment are needed, because this procedure has a higher complication rate than routine frontal sinus surgery. This stepwise, minimally invasive endoscopic approach to the failed FSO has been described with initial success rates between 81% and 93% with relatively short-term follow-up, and most failures can be revised endoscopically with success.
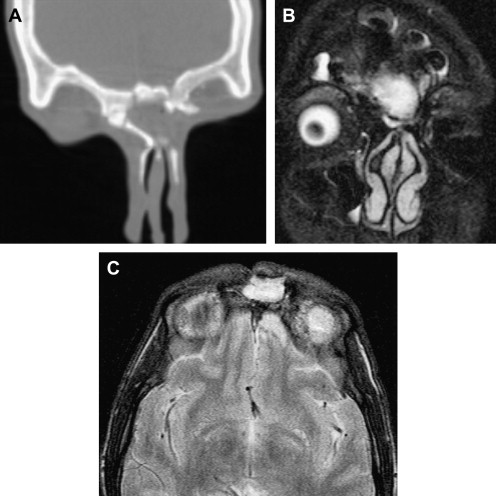
Although the frontal recess can typically be addressed from below, if loculated mucoceles are located laterally and unable to be reached endoscopically, a frontal sinus trephine can be used to marsupizalize the mucocele into the native frontal recess. In other cases, removing the inner sinus septum through frontal trephine or endoscopically can provide a route for drainage into the contralateral frontal sinus. Although this route is not anatomic, the inner sinus septectomy is often performed through an area that has not been traumatized by prior surgery, providing a way of safely ventilating the dysfunctional sinus (see Fig. 2 ).
The final option for reventilating the frontal sinus is a formal osteoplastic approach. This approach may be needed in cases of sinocutaneous fistulas, to excise the epithelialized fistula tract, or in conditions not amenable to simple trephine or endoscopic surgery, such as the need to remove alloplastic materials. Even these formal osteoplastic approaches can be performed with the intent to restore drainage of the dysfunctional sinus ( Fig. 6 ), and obliteration/ablation is not necessary simply because the approach to the sinus was through an open incision.
The final step in the surgical algorithm for the dysfunctional frontal sinus is a revision obliteration or ablative procedure, such as a Reidel procedure. In most series treating failed obliterations/ablations, more than 80% of patients can be successfully treated with procedures designed to restore ventilation, and fewer than one fifth require revision FSO or ablative operations. Even in these worst-case scenarios, high success rates are reported, although long-term follow-up is required to ensure success, because these radical procedures often take a decade or longer to fail.
Maxillary sinus
Dysfunctional maxillary sinuses are typically the result of failed Caldwell-Luc–type operations performed with the goal of stripping out sinus mucosa believed to be irreversibly diseased. Similar to external approaches to the frontal sinus, these radical destructive approaches often result in loculated mucoceles or infected pockets that are difficult to access through standard surgical techniques. In addition, this mucosal stripping leads to reactive, osteitic bone and a contracted sinus with a small lumen ( Fig. 7 ).