New instrumentation and techniques for endoscopic sinus surgery (ESS) are presently available that offer the potential of successfully treating recalcitrant chronic rhinosinusitis is a manner that minimizes operative times, sinus-mucosal trauma, and operative costs. This content describes current ESS techniques and quality-of-life outcomes, techniques for transnasal and transantral balloon catheter dilatation, and their outcomes. The authors address the changing medical climate that may open new avenues for surgeons to treat patients.
Since the early 1980s, endoscopic sinus surgery (ESS) has been widely used to treat recalcitrant chronic rhinosinusitis (CRS). Over the last 10 years, techniques and tools have emerged that offer targeted, minimally invasive therapy aimed at standardizing endoscopic sinus surgery, reducing operative time, and improving patient outcomes.
The minimally invasive sinus technique (MIST) was the first such effort designed to provide minimally invasive, targeted intervention to key areas within the sinuses. The basis of this minimally invasive technique is work done early by Messerklinger and his studies regarding mucociliary clearance. Minimally invasive sinus technique sought to standardize ESS by defining starting and ending points, minimizing mucosal trauma, and addressing four key areas within the sinuses.
More recent developments in the minimally invasive treatment of the sinuses include the use of balloon catheters that dilate the sinus ostia. Balloon catheter dilatation can be performed via two routes, transnasal or transantral, the later being more limited in capability. Both instruments, however, can be used to deliver minimally invasive targeted therapy to diseased sinuses.
Minimally invasive sinus technique
The minimally invasive sinus technique was originally described by Ruben Setliff and Peter Catalano as a means of surgically addressing CRS while at the same time fulfilling several of the supposed shortcomings of conventional endoscopic sinus surgery. Catalano describes MIST as a “targeted intervention” that is designed to address not the sinus ostia themselves but rather the transition spaces surrounding the sinus ostia. Fundamental to the philosophy of MIST is that the transition spaces are sources of CRS caused by mucosal contact when tissues become edematous, come into contact, and subsequently disrupt mucociliary transportion. The observations of Stammberger confirm that when these diseased transition spaces are cleared surgically, the more dependent sinuses (eg, maxillary, frontal) do demonstrate the capability of recovering function. This observation is the central tenant of MIST philosophy; therefore, the procedure is considered minimally invasive because of its specific intervention style. According to the authors, targeted intervention leads to less mucosal disruption, decreased discomfort, and decreased debridement requirements.
A second principle of MIST is the establishment of four landmarks, which reveal the key four transition spaces that need to be addressed during surgery. It is thought that these four transition spaces represent the contact points from where obstruction originates.
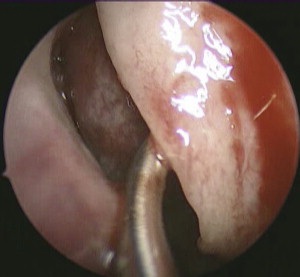
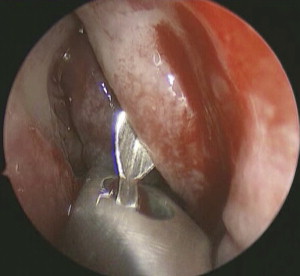
The first landmark is the uncinate process. The uncinate process, together with the hiatus semilunaris, leads to the first transition space, which is the infundibulum. During the MIST procedure, the uncinate process is removed using a technique described by Parsons. The uncinate process is fractured with a probe ( Fig. 1 ) and removed using a backbiting instrument ( Fig. 2 ) until the lacrimal bone is reached. The microdebrider, which is thought to be an atraumatic device because of its oscillating sharp teeth, is also used to resect the uncinate process. The agger nasi is exposed and the infundibulum is opened during this maneuver. The maxillary sinus ostium is not addressed, because opening the first transition space permits ventilation of the maxillary sinus and eventual recovery.
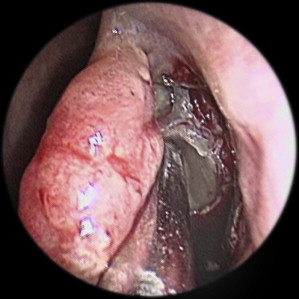
Ethmoid dissection is limited to the second landmark, which is the medial wall of the ethmoid bulla and the second space, or superior semilunar hiatus. Again, the microdebrider is used to remove the landmark and expose completely the second transition space ( Fig. 3 ). The lamina papyracea is identified as is the basal lamella. No further ethmoid dissection is performed at this point. The basal lamella is not perforated, and the posterior ethmoid sinuses are not dissected. The sphenoethmoidal recess is left unaddressed, and the sphenoid is not entered.
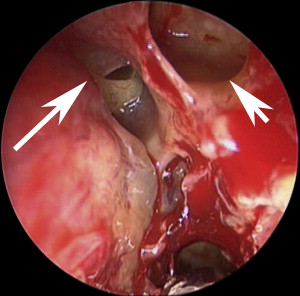
The completion of the procedure is performed by opening the third and fourth transition spaces. The third landmark (posteromedial wall of the agger nasi) and third space (frontal recess) are inspected ( Fig. 4 ). After this the fourth landmark (basal lamella) and fourth space (retrobulbar space) are identified and inspected. Catalano advocates that the agger nasi be taken down to improve frontal recess patency when required because clearance of the first, second, and third spaces in theory permit ventilation of the frontal sinus and improve mucociliary transport out of the frontal sinus. No specific manipulation of the frontal sinus is undertaken. When the procedure is completed, the middle meatus is not stented, or if necessary is filled with a bioabsorbable gel.
There are few studies that demonstrate outcomes when this technique is used. Quality-of-life surveys issued in early studies demonstrated improvements over baseline assessments. Elderly subjects undergoing this procedure reported an average of 84% improvement in quality of life. Catalano and Roffman prospectively treated subjects with the MIST protocol and assessed quality-of-life outcomes via the Chronic Sinusitis Survey over a period of 23 months. Significant improvements were noted in several domains, notably symptom scores, medication usage, mean total score. Forty percent of subjects reported quality-of-life levels that were comparable to control subjects. The Glasgow benefit inventory was used by Salama and coworkers to evaluate 143 subjects undergoing the MIST procedure. At 6 weeks, 12 weeks, 1 year, and 3 years following the procedure, significant reductions in nasal symptom scores and increases in total quality-of life scores were demonstrated.
There are no studies comparing outcomes of MIST with those of conventional functional endoscopic sinus surgery; therefore, no real conclusions can be drawn regarding the efficacy of one technique over the other. The only study that appears to compare on some level MIST and conventional endoscopic sinus surgery was one performed by Kuehnemund and colleagues. Sixty-five disease-matched subjects underwent limited (infundibulotomy, anterior ethmoidectomy, and maxillary antrostomy) or extended (sphenoethmoidectomy, frontal recess dissection, and partial middle turbinate resection) endoscopic sinus surgeries. The authors found identical outcomes in subjects when symptoms were assessed and saccharin transit times in both groups. The authors proposed that more conservative surgical approaches could produce adequate treatment results.
In clinical practice, MIST presents the surgeon with a limited and defined surgical intervention. The technique is easy to accomplish, has defined endpoints, and is easily tolerated by patients. Perhaps a significant drawback of conventional endoscopic sinus surgery is the lack of standardization. From another perspective, the limitations of MIST reveal its potential shortcomings. Ultimately, questions may arise regarding the treatment of a sphenoid sinus lesion or the posterior ethmoid sinuses if neither the superior meatus nor the sphenoethmoidal recess are manipulated. Additionally, in the treatment of diffuse hyperplastic disease, host factors and biofilms are not specifically addressed with this intervention. Nevertheless, the standardized technique presents the surgeon with a means of easily reproducing their approach and assessing personal outcomes. Additionally, patients can be offered clear expectations related to the extent of surgery.
The lack of outcomes data for MIST presents clinicians with a sizable challenge. All outcomes data in patients undergoing MIST is based on prospective, nonrandomized studies. Because a randomized prospective study between patients undergoing MIST and patients undergoing conventional endoscopic sinus surgery has not been performed to date, the knowledge gained from such a study would ultimately help to determine whether patients would be better served by one technique over the other.
Balloon catheter dilatation
History
In 2005, Acclarent, Inc (Melrose Park, CA, USA) introduced a transnasal balloon catheter dilatation system that could be used during endoscopic sinus surgery for the minimally invasive treatment of chronic sinus disease. More recently, ENTellus Medical (Maple Grove, MN, USA) introduced a balloon catheter system for treating the maxillary sinus and infundibulum via a canine fossa puncture that can be performed under local anesthesia or with minimal sedation. Although these devices have widely been considered novel instruments for the treatment of sinus ostia during endoscopic sinus surgery, the concept of balloon dilatation for the treatment of sinus disease is not new.
In 1947, Janse and Houser reported on the use of a “carefully lubricated and sterile finger cot” that was attached to a sphygmomanometer that was used to “distend the sinus openings into the meatus” to relieve the patient of several cranial neuralgias. Since that time, balloon catheters have been put to use for purposes with more sound medical bases: the repair of orbital floor fractures, the treatment of choanal atresia, and even the reduction and repair of a sphenoid sinus encephalocele and cerebrospinal fluid leak.
Newer forms of balloon catheters exist for the treatment of inflammatory sinus disease and treat the sinuses via two routes: transnasal and transantral. Although the routes of deployment differ, the principles underlying their benefit are the same.
Transnasal Balloon Catheter Dilatation
Since 2005, transnasal balloon catheter dilatation of the sinuses has been widely performed to surgically treat CRS. The system has three components: (1) guide, (2) guidewire, and (3) balloon catheter. The vehicle through which balloon catheter dilates the sinuses is the sinus guide catheter, which is a rigid translucent tube that is either curved (maxillary and frontal sinuses) or straight (sphenoid sinus) at the tip. After the catheter guide is chosen, a transillumination guidewire is threaded into the sinus. In the past, confirmation of entry into the sinus was exclusively performed with fluoroscopy. Studies have demonstrated that radiation dose to the patient and surgeon is low during use of fluoroscopy; however, transillumination removes these risks and can be performed in all three sinuses to confirm proper placement ( Fig. 5 ). A balloon catheter is inserted over the guidewire into the sinus. The balloon is inflated with saline or contrast material (if fluoroscopy is used). Inflation of the balloon results in fracture and dilation of the sinus ostia. Studies performed by Brown and Bolger confirm the feasibility of this technique.
Balloon dilation of the maxillary sinus is typically performed while using the 0-degree telescope. The middle turbinate is gently medialized to facilitate placement of the instrumentation. The uncinate process does not need to be removed; however, resection can facilitate proper placement of the sinus catheter guide. The catheter guide is inserted into the middle meatus at the junction of the superior two thirds and inferior one third of the maxillary line to accommodate the anatomic position of the maxillary sinus os ( Fig. 6 ). The guidewire is placed into the maxillary sinus where transillumination or fluoroscopy can be used to confirm entry. The ostium is then dilated using the balloon catheter. It is critically important to subsequently visualize the dilated ostium with a 45-degree or 70-degree telescope to confirm that the true ostium and not an accessory ostium was dilated to avoid a recirculation phenomenon, especially if the uncinate is preserved.
Balloon catheter treatment of the ethmoid sinuses is limited to deployment of a drug-eluting reservoir. The anterior ethmoid is punctured with a trocar and the reservoir is deployed ( Fig. 7 ). Currently, this reservoir is approved by the US Food and Drug Administration for use with saline only; however, trials are under way that are evaluating the effectiveness of passive delivery of triamcinolone acetate 40 mg/mL for chronic ethmoidal disease. If the ethmoid sinuses require surgical treatment for significant disease, either a limited or complete ethmoidectomy must be performed with conventional instruments. Balloon catheter dilation of the frontal sinus ( Fig. 8 ) can be done with or without previous ethmoidectomy. Similarly, a reservoir with triamcinolone acetate 40 mg/mL can be deployed within the frontal sinus to deliver topical therapy.
Surgical treatment of the sphenoid sinus is done under endoscopic visualization and confirmation of the illumination catheter in the floor of the sphenoid sinus. Using the straight catheter guide, the balloon is threaded through the sphenoethmoidal recess and is used to dilate the sphenoid sinus ostium.
Patient-selection criteria for transnasal balloon catheter dilation of the sinuses are not established. However, Friedman and Schlach detailed their experience with balloon catheter dilation of the sinuses and suggest the following: failed medical management including antibiotics, topical steroid sprays and allergy evaluation; persistently abnormal CT after treatment of 4 weeks; three or more episodes of recurrent sinus disease in 1 year; and critically ill patients for whom endoscopically derived cultures for fever of unknown origin are necessary. In their series, subjects had Lund-McKay scores less than 10. The authors suggest that patients who need revision surgery, have sustained significant trauma, have primary ciliary disorders, or extensive polyposis are less ideal candidates for transnasal balloon catheter dilation and would likely benefit more from conventional endoscopic sinus surgery with hand instruments.
Given its recent deployment, the outcomes following transnasal balloon catheter dilatation of the sinuses are limited to a few prospective, nonrandomized studies. Specific outcomes measured have included the ostial patency, Sino-nasal Outcomes Test 20 (SNOT-20) quality-of-life indices, endoscopic examination, and CT scores. Outcomes are reported primarily on a series of 109 subjects who underwent transnasal balloon dilatation of 307 sinuses and were followed over a period of 2 years. Outcomes were broken down into three follow-up studies. Initial reports from Bolger and colleagues revealed a patency rate of 80.5% (247 out of 307) with reductions in SNOT-20 scores from 2.25 down to 1.09. Kuhn and colleagues performed endoscopy on 66 of the original 109 subjects and noted that 172 out of 202 sinus ostia remained patent. Together with the 56 that underwent CT imaging, functional patency was determined to be 93.5% (86 out of 92) in the maxillary sinus; 86.1% (31 out of 36) in the sphenoid sinus; and 91.9% (68 out of 74) in the frontal sinus. After 2 years, SNOT-20 scores stabilized at 0.87 (2.17 at baseline) and Lund-MacKay scores changed from 9.66 preoperatively to 2.69 during this follow-up period. There is some dropout in this series; therefore, outcomes on several subjects and sinuses are unavailable for review.
The minimally invasive treatment of CRS with transnasal balloon catheters has several clinical and research implications. From a clinical standpoint, the use of transnasal balloon catheters presents an interesting option for patients with chronic or recurrent rhinosinusitis who desire surgical treatment but are concerned about having, or may not be candidates for, conventional endoscopic sinus surgery. For physicians, balloon catheters represent tools that can be used to potentially decrease operative time, decrease blood loss, and improve outcomes for patients. Furthermore, the ease by which balloon catheter dilatation can be performed raises the question of whether transnasal balloon catheter dilatation is suitable as an office-based procedure, either in the primary or in the revision setting. An example would be the completely stenosed sinus in patients who are symptomatic for whom dilatation could be performed in the office without requiring a general anesthetic.
The indications for use of transnasal balloon catheters, whether in the operating room or within the office, have yet to be clarified. Despite seemingly straightforward criteria proposed by Friedman and Schalch, transnasal balloon catheters may in fact be indicated in more severe disease. Catalano and Payne have recently published data regarding the efficacy of balloon dilatation of the severely diseased (eg, diffuse hyperplastic disease, frontal opacification, and Samter’s triad) to determine the utility of these tools in this patient subset. Subjects were not treated preoperatively with systemic corticosteroids and were excluded from the study if there was no postoperative follow-up or postoperative imaging. Overall, 14 out of 29 frontal sinuses demonstrated improvement in Lund-MacKay scores: 1.48 to 1.10. Of the remaining 15 frontal sinuses, three worsened. Subjects were followed for a minimum of 6 months and a maximum of 9 months. The short-term follow-up, uncertain dropout rate, and limited results do not help us determine whether the balloon is a useful instrument in severe disease, but it in some fashion does offer the potential to treat severe disease. Studies establishing patient criteria are, therefore, indicated.
Several unanswered questions present potential areas for clinical research. Although 2-year data is available regarding patients treated with transnasal balloon catheters, the long-term benefit of this technology is not yet known. There was a considerable dropout rate of the original cohort studied by Bolger and colleagues and data on missing subjects is not known. Long-term outcomes present the first consideration for long-term clinical research where balloon catheters are concerned.
Another issue to be considered is the cost of endoscopic sinus surgery with and without the use of the transnasal balloon catheters. Friedman and coworkers retrospectively reviewed the cost of transnasal balloon catheter dilatation compared with conventional endoscopic sinus surgery. In their analysis, the cost of using transnasal balloon catheters was compared with conventional endoscopic sinus surgery; however, when comparing revision endoscopic sinus surgery, data indicated a cost advantage to using balloon catheters. By their own criteria, subjects who were severely diseased were not included in the study, so it is unclear what the extent of disease was that required revision and why transnasal balloon catheter dilatation cost less in revision cases. This study could be expanded to be done in a prospective fashion, and incorporate the expense of postoperative debridement or cost of revision surgery. Furthermore, the cost of using balloon catheters in the outpatient setting and how reimbursement weighs against this cost would also be useful for clinical decision making.
There has been much research and discussion about the influence of osteitis in the pathogenesis of CRS. If osteitis were to play a significant role in the pathogenesis, a reasonable assumption would be that the osteitis needs to be addressed. The manner in which the osteitic bone needs to be addressed has not been clarified. Some advocate removal of as much osteitic bone as possible; however, others note that removal of certain osteitic bone is impractical. How well does balloon catheter dilatation succeed in patients with osteitis of the frontal recess or sphenoid sinus? If concomitant hybrid ethmoidectomies are performed, does osteitis of the anterior ethmoid and frontal recess occur in the long term?
Perhaps the biggest determinant of whether the use of balloon catheters represents an emerging technology that will survive the test of time is a yet-to-be-performed prospective study comparing ESS with transnasal balloon catheters to ESS with strictly conventional handheld or powered instruments. The randomized enrollment of patients who are similarly diseased into two treatment arms and comparing quality of life and surgical outcomes are the most effective means of demonstrating whether there has been selection bias in either group,. Comparison of outcomes with transnasal balloon catheters to historical outcomes of ESS with handheld or powered instruments.
Transantral Balloon Catheter Dilatation
The idea of the transantral canine fossa approach to dilate the maxillary antrostomy was developed by Entellus Medical (Maple Grove, MN) as the FinESS system ( Fig. 9 ).



