Purpose
To report a simple muscle transposition procedure without tenotomy or muscle splitting to treat abducens palsy.
Design
Retrospective, interventional, consecutive case series.
Methods
Nine patients with esotropia resulting from abducens palsy whose eyes could not abduct beyond the midline underwent this muscle transposition procedure, in which a suture was inserted through the temporal margin of each vertical rectus muscle. The same monofilament suture also was inserted into each inferotemporal or superotemporal sclera. The lateral margin of each vertical rectus muscle was transposed superotemporally or inferotemporally and was sutured onto the sclera. All 9 patients underwent unilateral muscle transposition, and 6 of the 9 underwent a medial rectus muscle recession combined with muscle transposition in the same eye.
Results
The surgical correction by muscle transposition alone ranged from 24 to 36 prism diopters, and that by muscle transposition and recession of the medial rectus muscle ranged from 50 to 62 prism diopters. The mean correction was 46.3 ± 13.1 prism diopters per eye. All paretic eyes could abduct beyond the midline. No major vertical ductional disturbances developed. Anterior segment ischemia did not occur in any patients.
Conclusions
This procedure, which achieved the same corrective results as other popular procedures, is simple to perform because it requires only a suture from the muscle to sclera. Tenotomy or splitting of the transposed muscles is unnecessary.
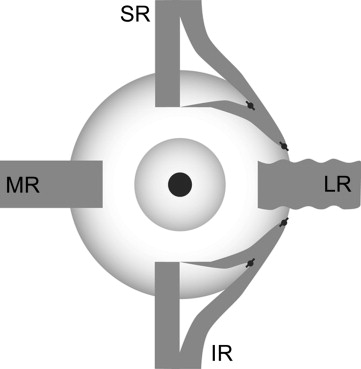
To correct esotropia resulting from abducens palsy, transposition of the healthy superior and inferior rectus muscles toward the paretic lateral rectus muscle should be performed, because strengthening of the paretic lateral rectus muscle by resection usually is ineffective. Various muscle transposition procedures for abducens palsy have been devised since 1908, when Hummelsheim first reported his procedure. Because most of muscle transposition procedures generally require tenotomy of the transposed muscles, there is a postoperative risk of anterior segment ischemia. Therefore in 1964, Jensen described a procedure that did not require tenotomy. That procedure is considered one of the safest, because it reduces the possibility of anterior segment ischemia; however, it requires splitting of 3 rectus muscles. Even in the procedure described by Jensen, anterior segment ischemia has been reported in some cases. In 2003, we reported a muscle transposition procedure in which the halves of the vertical rectus muscle bellies are sutured onto the sclera without either tenotomy of the vertical rectus muscles, as in the procedure of Hummelsheim, or surgical treatment of the lateral rectus muscle, as in the procedure of Jensen ( Figure 1 ). This procedure achieved postoperative results similar to those with previous procedures. However, we believed that splitting of the muscle could cause operative damage to the transposed muscles. To reduce operative damage further, in 2005, we reported 3 patients who underwent our second new muscle transposition procedure without tenotomy or splitting of the transposed muscles. Since then, the number of patients who have undergone that procedure increased. We report herein the postoperative results of this second new muscle transposition procedure.
Methods
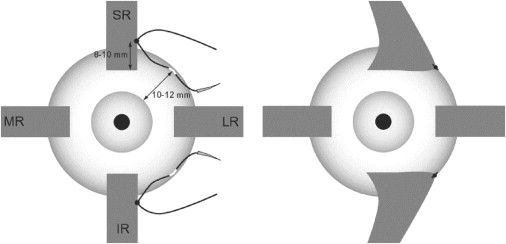
Shiga University of Medical Science Institutional Review Board approved the review of patient data for this retrospective study. Informed consent for our transposition procedure was obtained in a document from each patient, and the study followed the tenets of the Declaration of Helsinki. Figure 2 shows our current muscle transposition procedure. A 6-0 polypropylene monofilament fiber suture or a 5-0 polyester braided fiber suture was inserted through the temporal muscular margin of each vertical rectus muscle at approximately one third of the width from the edge at a distance of 8 to 10 mm behind the muscle insertion. Each suture carefully should be placed apart from the large vessels of each muscle to prevent anterior segment ischemia. The same suture also was inserted through each scleral wall at a distance of 10 to 12 mm behind the limbus at the superotemporal or inferotemporal quadrant. The lateral margin of each vertical rectus muscle then was transposed superotemporally or inferotemporally and was sutured to the sclera. We gave each patient a convincing explanation about our transposition procedure by using a detailed description with an illustration of the procedure.
Nine patients with abducens palsy whose eyes could not abduct beyond the midline underwent this muscle transposition procedure under general anesthesia at the hospital of Shiga University of Medical Science. In 6 of the 9 patients (67%), the recession of the medial rectus muscle was combined with the transposition procedure. The angle of squint in primary gaze at a distance of 5 m before and after muscle transposition was measured using the prism cover test or Krimsky prism test. The field of binocular single vision was measured on the Hess chart at 1 m.
Results
Table 1 shows the profiles of the 9 patients (5 men, 4 women) with abducens palsy. Six patients had abducens palsy unilaterally and 3 patients had bilateral disease. The cause of the abducens palsy was trauma in 4 patients, unknown in 4 patients, and congenital in 1 patient. The patient ages at surgery ranged from 31 to 66 years (mean ± standard deviation, 53.8 ± 9.6 years). The duration from onset to surgery ranged from 12 to 151 months (mean ± standard deviation, 36.0 ± 47.5 months), except for 1 patient (Patient 2) with congenital disease who had left abducens palsy at birth. She underwent strabismus surgery, that is, recession of the medial rectus muscle and resection of the lateral rectus muscle, at 22 years of age. The duration of the follow-up ranged from 1 to 89 months (mean ± standard deviation, 14.3 ± 28.3 months).
| Patient No. | Sex | Cause | Laterality | Age at Surgery (y) | Time from Onset to Surgery (mos) | Muscle Transposition | Medial Rectus Recession (mm) | Preoperative Comments |
|---|---|---|---|---|---|---|---|---|
| 1 | F | Trauma | B | 66 | 13 | L | L (8) | — |
| 2 | F | Congenital | L | 31 | — | L | NP | With previous surgery of LR resection and MR recession in left eye at 22 y of age |
| 3 | F | Trauma | B | 59 | 29 | R | R (6) | — |
| 4 | M | Unknown | R | 59 | 12 | R | NP | — |
| 5 | M | Trauma | R | 55 | 15 | R | R (3) | With traumatic optic neuropathy in right eye |
| 6 | M | Unknown | R | 50 | 151 | R | R (3) | — |
| 7 | M | Unknown | R | 56 | 17 | R | NP | — |
| 8 | F | Trauma | B | 54 | 39 | L | L (5) | — |
| 9 | M | Unknown | R | 54 | 12 | R | R (6) | — |
Muscle transposition was performed in all patients. Recession of the medial rectus muscle from 3 to 8 mm was combined with muscle transposition in the 3 patients with bilateral abducens palsy as well as 3 of the 6 patients with unilateral palsy.
Table 2 shows the preoperative and postoperative ocular deviation in primary gaze at distance. The preoperative deviation ranged from +70 to +75 prism diopters (PD) in 3 patients with bilateral paresis and from +24 to +66 PD in 6 patients with unilateral paresis (+ = esotropia; − = exotropia). The mean preoperative deviation in all patients was +52.2 ± 21.0 PD. The postoperative deviations 1 month after surgery ranged from +8 to +25 PD in 3 patients with bilateral palsy and from −20 to +10 PD in 6 patients with unilateral palsy. Only 1 patient with unilateral abducens palsy (Patient 5) had an exotropia after the unilateral muscle transposition combined with a medial rectus muscle recession. At the final examination, the postoperative deviation ranged from +8 to +25 PD in 3 patients with bilateral palsy and from −20 to +10 PD in the 6 patients with unilateral palsy. The same postoperative eye position was retained until the time of the final examination in all patients, although the follow-up duration in 5 patients was less than 6 months. The mean ocular deviation in all 9 patients improved from +52.2 ± 21.0 PD before surgery to +5.9 ± 12.9 PD after surgery. The ocular deviations corrected by the muscle transposition procedure alone ranged from 24 to 36 PD and those by the muscle transposition procedure combined with the recession of the medial rectus muscle ranged from 50 to 62 PD. The mean correction in all 9 patients was 46.3 ± 13.1 PD.
| Patient No. | Palsy | Preoperative Deviation (PD) | Deviation 1 Month after Surgery (PD) | Deviation at Final Examination (PD) | Corrected Deviation (PD) | Follow-up Duration after Surgery (mos) | Postoperative Comments |
|---|---|---|---|---|---|---|---|
| 1 | Bilateral | +75 | +25 | +25 | 50 | 1 | Declined additional surgery |
| 2 | Unilateral | +24 | 0 | 0 | 24 | 89 | — |
| 3 | Bilateral | +75 | +20 | +20 | 55 | 3 | With additional surgery of MR recession of 6 mm in left eye 3 mos later |
| 4 | Unilateral | +30 | 0 | 0 | 30 | 9 | — |
| 5 | Unilateral | +30 | −20 | −20 | 50 | 11 | — |
| 6 | Unilateral | +60 | +8 | +6 | 54 | 9 | — |
| 7 | Unilateral | +40 | +4 | +4 | 36 | 1 | — |
| 8 | Bilateral | +70 | +8 | +8 | 62 | 2 | SBV regained with prism glasses |
| 9 | Unilateral | +66 | +10 | +10 | 56 | 4 | SBV regained with face turn to right |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


