Fig. 6.1
Inferior conjunctivochalasis
The primary indication for surgical intervention for conjunctivochalasis is intolerance of foreign body sensation. The most common locations of excess conjunctiva causing symptoms include inferiorly and inferotemporally. Patients often report foreign body sensation or localized epiphora sensation in that region of their eyes. The following section describes various techniques to remove the excess conjunctiva. Although some studies have been published comparing techniques, there is no strong evidence in the literature that one surgical technique is substantially better than the other. Most surgeons choose one or two techniques based on their comfort level and make modifications based on their individual post-op results.
6.3.1 Surgical Options
Conjunctivochalasis resection
Pros
Reapproximates normal conjunctival anatomy
Cons
Requires suture placement
Steps: Anesthetize the eye with topical proparacaine eyedrops. Prep and drape the eye and insert a lid speculum. Inject 1 % lidocaine in the inferior subconjunctival region. Make an arc-like incision in the inferior bulbar conjunctiva approximately 2 mm from the corneal limbus. Excise the subconjunctival tissues distally from the arc-like incision to the extent of the redundant conjunctiva. Make radial incisions to divide the conjunctiva into nasal, central, and temporal blocks. Resect the redundant conjunctiva in each block based on the extent of redundancy. Close the central block first, using 8-0 Vicryl interrupted sutures. The remaining two blocks should be sutured closed with adjustments to maintain appropriate shape and tension for smooth junctions between the blocks and to obtain a good tear meniscus. Prescribe topical 0.5 % levofloxacin and 0.1 % fluorometholone eyedrops for 1 month. Remove stitches at 1 week postoperatively (Hara et al. 2011).
Conjunctivochalasis resection with cautery
Pros
Better adherence of conjunctiva because of cautery
Cons
Theoretically increased scarring because of cautery
Removal of nylon suture required
Steps: Anesthetize the eye with topical proparacaine eyedrops and subconjunctival 2 % lidocaine. Use ophthalmic microscissors to make a semicircular incision from 3 o’clock to 9 o’clock position in the inferior conjunctiva approximately 0.5 mm from the corneal limbus. Leave angle of 45° at the two ends of the incision. Use an iris repository and microforceps to push the loose conjunctiva from the inferior fornix onto the corneal surface. The redundant conjunctiva will be seen overlapping onto the inferior corneal surface. Make a second curved incision into the redundant conjunctiva and parallel to the first incision. This creates a semiperitomy strip of redundant conjunctiva that should be excised in close proximity to the 0.5-mm conjunctiva flap adjacent to the inferior corneal limbus. Place gentle cautery in two lines (12–18 spots in zigzag pattern) subconjunctivally under the incision to form tight adhesions with the underlying sclera along the corneal limbus. Use 10-0 nylon suture to close the incision at 3 o’clock and 9 o’clock positions. Remove the sutures at 1 week postoperatively (Wang et al. 2012).
Conjunctival resection with paste-pinch-cut technique
Pros
Possible decrease in intraoperative time because it does not require suturing
Similar technique to modern pterygium excision with autograft
Cons
Risk of glued wound becoming unsealed
Tip
Immediately after injection of the thrombin sealant, use modified (curved) ptosis forceps to pinch the conjunctiva and hold for 20 s. This step gathers the excess conjunctiva and subconjunctiva sealant into a ridge and allows the sealant to polymerize.
Steps: Anesthetize the eye with topical proparacaine eyedrops. Prep and drape the eye and insert a lid speculum. Inject 2 % lidocaine with epinephrine in the inferior subconjunctival region. Use a methylene blue pen to place an arc-like marking approximately 5–6 mm inferior to the limbus. Use Westcott scissors to make a small buttonhole in the temporal bulbar conjunctiva at the edge of the pen marking. Use a 19-gauge cannula to inject 0.3 ml of the fibrinogen component of fibrin sealant (Tisseel; Baxter AG Industries, Vienna, Austria) through the buttonhole subconjunctivally along the pen marking. Inject 0.3 ml of the thrombin component in a similar fashion. Immediately after injection of the thrombin sealant, use modified (curved) ptosis forceps to pinch the conjunctiva and hold for 20 s. This step gathers the excess conjunctiva and subconjunctiva sealant into a ridge and allows the sealant to polymerize. After 20 s, use Westcott scissors to excise the ridge, leaving a sealed wound 2–3 mm inferior to the limbus. Prescribe antibiotic eyedrops to use three times a day for 1 week and steroid eyedrops to use three times a day for 3 weeks. Schedule follow-up appointments at 1-day, 1-month, and 3-month intervals (Doss et al. 2012).
Conjunctival resection with sutured amniotic membrane transplantation
Pros
Reapproximates normal conjunctival anatomy
Cons
Requires suture placement
Cost of amniotic membrane graft
Steps: Anesthetize the eye with topical proparacaine eyedrops. Prep and drape the eye and insert a lid speculum. Inject 2 % lidocaine with epinephrine in the inferior subconjunctival region. Make a peritomy of the inferior conjunctiva 1 mm from the limbus. Use Westcott scissors to excise the loose and redundant conjunctiva. Place amniotic membrane transplant over the conjunctival defect and trim off excess membrane. Place a continuous suture using 10-0 nylon to approximate the conjunctival edges with the amniotic membrane. Place a mixed antibiotic steroid ointment into the operative eye and then patch the eye. Remove the eye patch on postoperative day one. Prescribe artificial tears, steroid, and antibiotic eyedrops to use five times a day until full epithelialization of the amniotic membrane, which usually occurs in 2 weeks. Remove the suture at 2 weeks postoperatively. Discontinue steroid and antibiotic eyedrops 3–4 days after suture removal. Continue artificial tears for at least 1 month (Georgiadis and Terzidou 2001).
Conjunctival resection with fibrin glue amniotic membrane transplantation
Pros
Possible decrease in intraoperative time because it does not require suturing
Similar technique to modern pterygium excision with allograft
Cons
Risk of glued wound becoming unsealed
Steps: Anesthetize the eye with topical 2 % lidocaine gel and a few drops of non-preserved 1:1,000 epinephrine for hemostasis. Prep and drape the eye and insert a lid speculum. Make an arc-like inferior conjunctival peritomy 1–2 mm posterior to the limbus. Place traction suture using a 7-0 Vicryl placed 2 mm posterior to the limbus at 6 o’clock position and rotate the eye upward. Look for loose conjunctiva that is easily mobile using forceps. Trim off areas of severely thinned conjunctiva. Apply the amniotic membrane over the conjunctival defect, with the membrane stromal side toward the sclera. Fold back half of the amniotic membrane. Apply thrombin solution to the sclera surface, and apply fibrinogen solution to the stromal surface of the membrane. Flip the membrane back onto the sclera and use a muscle hook over the membrane to spread the fibrin glue that is under the membrane. Repeat the above steps for the other half of the amniotic membrane. Trim the excess amniotic membrane and fibrin so that the membrane is flush with the conjunctiva (Kheirkhah et al. 2007).
Tip
Apply thrombin solution to the sclera surface and apply fibrinogen solution to the stromal surface of the membrane. Flip the membrane back onto the scleral and use a muscle hook over the membrane to spread the fibrin glue that is under the membrane.
No conjunctival resection/suture-only technique
Pros
No conjunctival excision required
Cons
Risk of globe perforation when suturing excess conjunctiva to sclera
Tip
The normal anatomic depth of the inferior fornix is 8 mm from the limbus. Avoid going farther than 8 mm, as restriction of lower gaze may occur.
Steps: Anesthetize the eye with topical proparacaine eyedrops. Prep and drape the eye and insert a lid speculum. Inject 2 % lidocaine with epinephrine in the inferior subconjunctival region. Place three interrupted 6-0 Vicryl sutures 8 mm posterior from the limbus, attaching the bulbar conjunctiva to the sclera. Take care not to perforate the globe. The normal anatomic depth of the inferior fornix is 8 mm from the limbus. Avoid going farther than 8 mm, as restriction of lower gaze may occur. Vicryl suture is ideal for this procedure because it permits focal inflammation to occur so that the forniceal conjunctiva will firmly attach to the globe (Otaka and Kyu 2000).
Lower eyelid malpositions, such as ectropion and entropion, can create either a dry eye syndrome or symptomatic epiphora. Corneal exposure from ectropion or irritation from lashes touching the cornea in entropion creates corneal irritation with a constellation of dry eye symptoms. Epiphora can result from reflex hypersecretion but can also occur from lacrimal pump failure or the inability of tears to enter a malpositioned or stenotic punctum. Lower eyelid malposition, whether ectropion or entropion, is commonly caused by involutional changes most commonly related to aging. Repair of these malpositions involves tightening the horizontal eyelid supports, namely, the tarsus and lateral canthal tendon. Repair of a dehiscent lower eyelid retractor band can restore vertical support in the eyelid and restore the tarsus to a favorable anatomic position. Techniques for managing involutional lower eyelid malpositions are summarized below and may be addressed by the general ophthalmic surgeon.
Floppy eyelid syndrome represents a pathologic end spectrum of involutional eyelid disease and may require special techniques and experience. Eyelid malpositions related to scarring (cicatricial disease) should be surgically managed in a significantly different manner. Skin disorders that result in skin tightening (i.e., scleroderma, burns, radiation) frequently cause ectropion, while conjunctival scarring diseases (i.e., Stevens-Johnson syndrome, trachoma, ocular cicatricial pemphigoid) cause entropion or trichiasis. In many cases, the management of cicatricial malpositions requires the addition of the deficient eyelid lamella, namely, skin for ectropion and mucous membrane for entropion, which are beyond the scope of this manual. Cicatricial changes from overcorrected ptosis repair or lower eyelid blepharoplasty may have scarring in more than one lamella and can be challenging. The approach of these cicatricial malpositions is not described below, and these patients warrant a referral to an ophthalmic plastic surgeon.
Indications for surgical intervention in lower eyelid malpositions include horizontal lower eyelid laxity, corneal decompensation from eyelashes rubbing against corneal surface, or persistent epiphora. Although some studies have been published comparing techniques, there is no strong evidence in the literature that one surgical technique is substantially better than the other. Most surgeons choose a technique based on their comfort level and make modifications based on their individual post-op results.
6.3.2 Surgical Options
Ectropion repair via formal lateral tarsal strip procedure
Pros
Good visualization of tarsus to attach to periosteum for better reapproximation and creation of new lateral canthal angle
Cons
More time intensive
Steps: Inject 2 % lidocaine with 1:100,000 epinephrine to the lower eyelid. Prep and drape the eye. Instill tetracaine and place a corneal protector. Make a 1-cm lateral canthotomy incision using a No. 15 Bard-Parker blade. Use straight scissors to perform an inferior cantholysis. Pull the lower eyelid laterally and use a marking pen to indicate the target amount of horizontal shortening. Resect the epithelium overlying the lid margin of the planned tarsal strip. Use scissors to divide the eyelid into two lamellae at the gray line. Remove the skin of the anterior lamella to expose the tarsus. Cut the conjunctiva along the inferior edge of the tarsus to create a strip of tarsus. Remove the conjunctiva from the newly created tarsal strip with scalpel or Beaver blade. Place a suture using 5-0 Vicryl or 4-0 Prolene to attach the tarsal strip to the internal lateral orbital periosteum at a slight angle so that it is a little higher compared to the height of the corresponding medial canthus. Approximate the upper and lower eyelid margins laterally using interrupted sutures. Close the canthotomy incision with absorbable sutures. Remove the corneal protector, either at completion of the procedure or prior to tying the canthal suspension suture. Apply ophthalmic antibiotic ointment to the incision site for 1–2 weeks (Anderson and Gordy 1979; Tse and Negg 2001).

Fig. 6.2
A lateral canthotomy and inferior cantholysis have been made

Fig. 6.3
Retract the eyelid laterally to estimate the horizontal redundancy in the eyelid
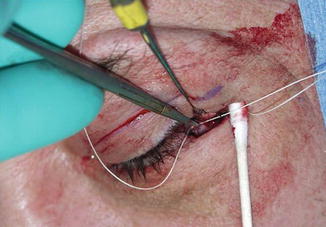
Fig. 6.4
Pass the Prolene suture in a medial to lateral direction to engage the internal orbital rim periosteum. Use a cotton-tipped applicator to protect the orbital tissue and a retractor to gently lift upward the upper limb of the canthal tendon for better exposure

Fig. 6.5
The canthal angle should be sharp, with the two gray lines in apposition
Tip
Orient scissors in correct angle when making full-thickness block excision of the redundant excessive eyelid to ensure better cosmetic result of new lateral canthal angle.
Steps: Inject 2 % lidocaine with 1:100,000 epinephrine to the lower eyelid. Prep and drape the eye. Instill tetracaine and a corneal protector. Make a 1-cm lateral canthotomy incision using a No. 15 Bard-Parker blade. Use straight scissors to perform an inferior cantholysis. Retract the eyelid laterally to estimate the horizontal redundancy in the lid with care to avoid excessive lengthening of the medial canthal tendon. Use straight scissors for a full-thickness block excision of the redundant excessive eyelid. Achieve hemostasis with cautery. Engage the cut tarsal edge with a 5-0 Prolene or 5-0 Vicryl. With retraction of the upper limb of the canthal tendon and protection of the orbital tissue with cotton-tipped applicator or small malleable retractor, pass the Prolene suture in a medial to lateral direction to engage the internal orbital rim periosteum. A sharp canthal angle can be reformed by adding a chromic suture which brings the two gray lines into apposition in the open canthotomy wound prior to tying the Prolene canthal suspension suture. Close the canthotomy incision with absorbable sutures. Remove the corneal protector, either at the end of the procedure or prior to tying the canthal suspension suture. Apply ophthalmic antibiotic ointment to the incision site for 1–2 weeks (Tse and Negg 2001).
Entropion repair, anterior approach
Pros
Quick procedure
Cons
Skin incision gives potential for visible scar and scleral show.
Steps: Inject 2 % lidocaine with 1:100,000 epinephrine to the lower eyelid. Prep and drape the eye. Instill tetracaine and place the corneal protector. Make a subciliary incision 2–3 mm below the eyelash line from a point inferior to the punctum to the lateral canthus and connect it to a canthotomy incision. Separate a skin-muscle flap away from the posterior lamella. Perform a horizontal tightening procedure as indicated above. Verify hemostasis. If dehiscence of the retractor band is noted, repair of the retractors to the inferior border of tarsus may be indicated. Redrape the skin-muscle flap of the lower eyelid and excise the excess. Close the subciliary-canthotomy incision with absorbable suture. Remove the corneal protector, either at the end of the procedure or prior to tying the canthal suspension suture. Apply ophthalmic antibiotic ointment to the incision site. Remove the sutures at 1 week postoperatively (Kronish 2001).
Entropion repair, posterior approach
Pros
Horizontal incision is done transconjunctivally.
Cons
More time intensive
Steps: Inject 2 % lidocaine with 1:100,000 epinephrine to the lower eyelid. Prep and drape the eye. Instill tetracaine and a corneal protector. Perform canthotomy incision, cantholysis, and resection/preparation for horizontal tightening as indicated above. Visualize the posterior lamella with retraction. Look for the common dehiscence of the retractor band. Use Westcott scissors first as a blunt dissector and then as scissors to make a horizontal conjunctival incision. If conjunctiva is excessive, a thin strip may be trimmed to the inferior pole of tarsus. Reattach the retractor band to the inferior pole of tarsus to bring the tarsus back into proper vertical orientation with 6-0 Vicryl sutures on a spatulated needle. Resuspend the eyelid via a horizontal tightening procedure of choice as above. Close the canthotomy incision with absorbable sutures. Remove the corneal protector, either at the end of the case or prior to tying the canthal suspension suture. Apply ophthalmic antibiotic ointment to the incision site for 1–2 weeks (Dresner and Karesh 1993; Kronish 2001; Tse and Negg 2001).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


