Well-differentiated thyroid cancer (DTC) carries an excellent prognosis. Although long-term survival rates are high, regional lymph node metastases are common. Surgical management of cervical lymph nodes is integral to the comprehensive treatment of DTC, but data from large randomized trials do not exist to define optimal treatment. Therapy is thus guided by observational data, and founded on an understanding of the behavior of lymphatic metastases in DTC. This article focuses on the significance of lymph node metastases in thyroid cancer, and the strategy for surgical management.
Approximately 37,200 people are expected to be diagnosed with thyroid cancer in the United States this year. Prognosis largely depends on the degree of tumor differentiation. In contrast to anaplastic tumors, well-differentiated thyroid cancer (DTC), including papillary and follicular carcinomas and their subtypes, has an excellent prognosis. Although long-term survival can exceed 90%, regional lymph node metastases are common and contribute significantly to morbidity. Surgical management of cervical lymph nodes is integral to the comprehensive treatment of DTC. Unfortunately, data from large randomized clinical trials do not exist to aid in defining optimal surgical treatment. The choice of surgical strategy is thus founded on a thorough understanding of the behavior and significance of lymphatic metastases in DTC and guided by observational data.
Background
Differentiated Thyroid Cancer Growth and Spread
The malignant behavior of well-differentiated thyroid cancer is characterized by varying degrees of local invasion, lymphatic infiltration, and hematogenous dissemination. Papillary thyroid cancers (PTCs) compose 77% of thyroid malignancies and demonstrate a strong propensity for regional nodal involvement. The most recent analysis of Surveillance, Epidemiology and End Results (SEER) data, including more than 33,000 patients with DTC, reports a 22% incidence of lymphatic involvement at initial operation in patients with PTC. Extrathyroidal extension was less common, involving 15% of patients, and distant metastases affected only 1% of patients at diagnosis. Other studies demonstrate lymphatic metastases in up to 50% of patients with DTC, depending on the timing of evaluation and diagnostic criteria.
In contrast to PTCs, follicular thyroid cancers (FTCs) are less common, with a low rate of lymphatic involvement but more frequent distant metastasis. According to SEER data, 10% of patients with FTC present with extrathyroidal spread, 3% with distant metastases, and only 2% with lymphatic involvement.
Anatomy of Cervical Lymphatics
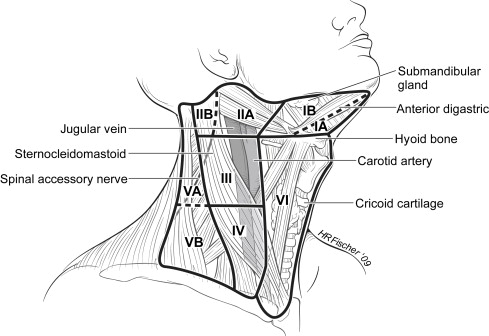
The thyroid gland is seated amid a rich lymphatic network. The cervical lymph nodes are divided into levels I to VI and grouped into central and lateral compartments ( Fig. 1 ). Level I nodes are submental and submandibular. Levels II to IV consist of the upper, mid-, and lower jugular nodes, respectively, with level V nodes lateral to the jugular groups in the posterior triangle. The pretracheal, paratracheal, and prelaryngeal (delphian) nodes compose level VI. Level VII lymph nodes are located in the superior mediastinum inferior to the sternal notch. Although not technically included in the cervical lymphatic system, the superior mediastinal group is another common site of DTC metastasis. Further subdivision of the levels I, II, and V nodes has been proposed based on significant anatomic landmarks. Ia refers to submental nodes whereas Ib nodes are submandibular. Level II is divided into superior (IIa) and inferior (IIb) nodes by the spinal accessory nerve, with IIb lateral to the nerve. Level Va is located superior to the level of the cricoid cartilage and Vb inferior. The spinal accessory nerve divides Va into inferior and superior sublevels. Grouping adjacent nodal levels together has practical application. Levels II to V compose the lateral or posterolateral compartment, whereas level VI is synonymous with the central or anterior compartment.
Patterns of Nodal Metastases
Several studies of cervical metastases in thyroid cancer suggest a general pattern of lymphatic spread from medial to lateral in the ipsilateral, then contralateral, neck. The incidence of nodal involvement is higher in the central compartment than the lateral compartment. Jugular lymph node metastases occur with greater frequency than do supraclavicular lymph node metastases, and involvement of submental or submandibular nodes is rare. Contralateral lymph node metastases greater than 1 cm have been described in 25% of patients with PTC. The majority of contralateral metastases are found in the central rather than lateral compartment. Mediastinal lymph node involvement is rare, occurring in only 5% of node-positive patients with PTC.
Incidence and location of nodal metastasis is ideally studied in a representative cohort of patients with thyroid cancer who undergo complete bilateral modified radical neck dissection (MRND) regardless of clinical node status. Mirallie and colleagues examined 119 patients with PTC who underwent bilateral cervical neck dissection, excluding only node-negative patients with microcarcinomas less than 1 cm in diameter: 60.5% of patients were found to have cervical lymph node metastases. Of node-positive patients, 83% had central, 61% had midjugular, 36% had supraclavicular, and 28% had subdigastric involvement on the ipsilateral side. Contralateral involvement in the paratracheal nodes occurred in 35% of node-positive patients, with contralateral jugular metastases in less than 25%. DTC metastases are thus most common within the central compartment; they are also frequent in the ipsilateral jugular groups. Contralateral involvement is less likely but nonetheless affects a significant proportion of patients.
Although central and jugular involvement is common, several studies have suggested infrequent involvement of levels I, IIb, and V. A series of 52 patients with lateral metastases at initial diagnosis who underwent MRND identified lymph node metastases by neck level. Levels IIa, III, and VI were each involved in more than 70% of patients. Involvement of other levels was significantly less common: only 16.7% of patients had positive nodes at level IIb, 13% at Vai, and 3.7% at Vb and Ib; there was no involvement of Vas. Level Ia was not dissected. Involvement of Level Ib, IIb, or V was associated with multilevel disease in all cases. In contrast, another small series reported positive nodes above the spinal accessory nerve (level I or IIb) in 21% of 34 patients; nearly half of those had no involvement of level IIa.
Many investigators have also described a relationship between the location of the cancer within the thyroid and the location of involved nodes. Quabain and coworkers prospectively studied a population of patients with DTC who underwent prophylactic MRND and were staged as pN0 by standard histopathology. Micrometastatic disease was identified by immunohistochemistry in 53% of the 80 patients enrolled, primarily occurring in those with tumors larger than 1 cm. Examination of the location of micrometastases indicated a tendency for upper-pole lesions to metastasize to more superior nodes, with isthmus and lower-pole lesions metastasizing to inferior nodes. Within the central compartment, all micrometastases occurred ipsilateral to the tumor unless the tumor was within the isthmus.
Despite the general pattern of medial to lateral spread, skip metastases—lateral compartment metastases without central compartment involvement—occur in a significant proportion of patients ( Table 1 ). In the study by Qubain and coworkers, 7% of patients with DTC micrometastases had lateral compartment involvement without evidence of central disease. In a prospective series of 52 patients with DTC and clinically positive lateral nodes who underwent MRND, 5 patients (9.6%) had no evidence of central compartment disease. Machens and colleagues examined 215 patients with thyroid cancer and lateral or mediastinal metastases and found skip metastasis in 19.7% of patients with PTC and 0 of 8 patients with FTC. A statistically significant inverse correlation was observed between the incidence of skip metastases and the number of positive lymph nodes. The presence of skip metastases was not significantly associated with tumor size or patient demographic characteristics.
| I | Ia | Ib | II | IIa | IIb | III | IV | V | Vai | Vas | Vb | VI | Skip Mets b | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pingpank (n = 44) | 38 | — | — | 49 | 43 | 21 | 76 | 59 | 28 | — | — | — | ||
| Roh (n = 52) | — | — | 4 | 72 | 17 | 72 | 76 | 13 | 0 | 4 | 90 | 10 | ||
| Yanir (n = 27) | — | — | — | 54 | — | — | 68 | 57 | 20 | — | — | — | 95 | 5 |
| Mirallie (n = 72) | — | — | — | 28 | — | — | 61 | 61 | 36 | — | — | — | 83 | 17 |
| Average | 38 | — | 4 | 39 | 59 | 19 | 68 | 64 | 31 | 13 | 0 | 4 | 88 | 12 |
a Values indicate the % of patients with positive lymph nodes at each level.
b Metastases to lateral nodes without evidence of central compartment involvement.
Risk Factors for Initial Nodal Metastases and Nodal Recurrence
Several risk factors have been defined for nodal involvement in DTC ( Table 2 ). At the time of initial treatment, patients with PTC and those younger than 45 years old are more likely to have lymph node metastases than their older counterparts or those with FTC. Patients with distant metastases are also more likely to harbor nodal metastases. Correlation between tumor size and lymph node metastases has been variably reported. Patients with tumors larger than 4 cm are 2 to 6 times more likely to have lymph node metastases present at operation than those with smaller tumors. In smaller tumors, the presence of lymph node metastases at initial operation correlated more strongly with vascular and soft tissue invasion than primary tumor size (<1 cm vs 1–2 cm). Locally invasive primary tumor and pronounced elevation in thyroglobulin levels have also been identified as possible risk factors. Patient and tumor characteristics associated specifically with mediastinal lymph node involvement include older age at diagnosis, poor tumor differentiation, more positive lymph nodes, and distant metastases.
| At Presentation | Recurrence |
|---|---|
| PTC | Male > female |
| Distant metastases | Extrathyroidal extension |
| Age <45 years | Age >55 years |
| Large tumor | Large tumor |
| Extrathyroidal extension | Macroscopically positive |
| Vascular invasion | Lymph nodes at initial operation |
| Elevated thyroglobulin |
Several risk factors are associated with regional lymph node recurrence in DTC. Male gender and extrathyroidal extension of the primary tumor have been implicated by several studies. Older age, larger tumor, and macroscopically involved nodes at initial surgery also are cited.
Ito and colleagues proposed a scoring system to stratify patients in terms of risk for lymph node recurrence, assigning 1 point each for
- ■
Age older than 55 years
- ■
Male gender
- ■
Massive extrathyroid extension
- ■
Tumor greater than 3 cm.
Patients with 0 points had a 10-year, lymph node disease-free survival of 98.4%. This declined in a stepwise fashion to 64.7% for patients with all 4 criteria.
Detection and Diagnosis
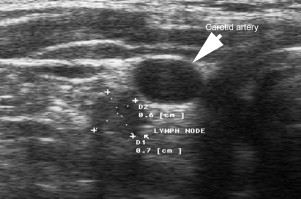
Regional metastases are routinely detected by physical examination and imaging studies. In the setting of a negative preoperative evaluation, unanticipated lymphatic metastases are also frequently discovered at thyroidectomy. Initial assessment for lymphadenopathy is by physical examination of the neck. The accuracy of this method varies with clinician experience and patient body habitus, but false-positive and -negative rates of 20% to 30% are reported. Clinician and patient factors also affect the accuracy of ultrasonography; however, ultrasound may detect cervical lymph node metastases in up to 34% of patients with a negative physical examination ( Fig. 2 ). Reported sensitivities for ultrasound in diagnosis of lymphatic metastases in DTC are widely variable, ranging from 10% to 92%. Specificity, as confirmed by fine-needle aspiration (FNA), is high, with a reported range of 89% to 99%. The sensitivity of ultrasound is particularly limited in the central compartment due to the presence of the trachea and thyroid gland. In patients whose thyroid gland remains in place, the false-negative rate for ultrasound detection of central compartment lymph node metastases is 36%. This rate drops to 18% for patients whose thyroid gland is surgically absent. Positive or indeterminate findings on physical examination or imaging can be evaluated with FNA, particularly if the presence or absence of malignancy influences the choice of surgical procedure.
Significance of lymph node metastases
The impact of lymph node metastases on survival in DTC has yet to be unequivocally defined. Nonetheless, lymphatic involvement is well established as a predictor of locoregional recurrence and implicated as a harbinger of distant metastases.
Locoregional Recurrence
Lymph node metastasis is described as a risk factor for locoregional recurrence in several observational studies. A retrospective review of 700 patients with DTC demonstrated a relative risk of recurrence of 4.2 in patients with lymph node metastases as compared with those without. This difference existed independent of treatment and other tumor and patient factors. Similarly, McHenry and colleagues reported recurrence of DTC in 19% of patients with initially positive nodes and 2% in node-negative patients after thyroidectomy and MRND.
Similar results are reported in series of patients with PTC only. According to a retrospective study by Salvesen and colleagues, initial node-negative status in patients with PTC predicted recurrence-free survival with a hazard ratio (HR) of 3.6. Ninety percent of N0 patients were disease-free 10 years after resection compared with 65% of patients who presented with positive lymph nodes. Wada and colleagues compared the rates of recurrence and mortality in 231 patients who had PTC with and without palpable lymphadenopathy. All patients underwent thyroidectomy and MRND; only a small minority received radioactive iodine postoperatively. The overall HR for disease-free survival in patients without palpable lymphadenopathy compared to those with nodal disease detectable on physical examination was 14.9 by multivariate analysis. The effect of lateral involvement was stronger than that of central compartment disease.
There are fewer studies exclusively concerned with nodal metastases in FTCs. Two retrospective reviews examined the effect of initial node-positive status on subsequent recurrence after total thyroidectomy with central lymph node dissection (CLND) and radioactive iodine therapy. Of patients who were initially node positive, 80% developed recurrence whereas only 34% of node-negative patients developed recurrence. This difference remained statistically significant on multivariate analysis.
The effect of nodal involvement is more pronounced in certain subgroups of patients with DTC. A retrospective review of 342 patients with PTC revealed nodal status as a statistically significant predictor of recurrence and survival in patients with T1, T2, and T3 tumors but not in patients with T4 tumors. In a study of patients with small DTC less than 2 cm, 20-year disease-free survival was 71% in N0 patients versus 56% in initially node-positive patients ( P = .02).
Distant Metastases
Nodal metastases have been identified as a predictor of systemic disease. In the series by McHenry and colleagues , 6% of patients with nodal involvement and 0.1% of patients without nodal involvement developed distant metastases. In another series stratified by tumor size, 0.7% of patients initially T1-T3N0 had distant metastases at diagnosis and 2.9% eventually developed distant spread. For T1-T3N1 patients, 8.5% had systemic involvement at diagnosis, and 15.1% later developed systemic disease. Reflexively, patients with metastatic disease are more likely to have lymphatic involvement. Analysis of 231 patients with PTC who underwent MRND revealed a significantly higher burden of positive regional lymph nodes, particularly lateral nodes, in patients with systemic metastases. These studies suggest that nodal involvement is reflective of more advanced or aggressive DTC.
Survival
Lymph node metastases have not traditionally been associated with mortality in DTC; however, recent evidence is accumulating to suggest decreased long-term survival in patients with lymphatic involvement. At least 6 case series have demonstrated no significant mortality risk associated with lymph node metastases in DTC. In contrast, a large, population-based, nested case-control study of all patients diagnosed with DTC in Sweden over 30 years suggests that lymph node metastases are associated with increased mortality. In a multivariate analysis controlling for TNM stage, the odds ratio for DTC-related death was 1.9 in patients with lymphatic involvement compared with those without. Analysis of SEER data from more than 19,000 patients demonstrated a statistically significant survival difference in patients with DTC based on nodal status. The 14-year survival was 82% in node-negative patients versus 79% in node-positive patients. A more recent review of SEER data from more than 33,000 patients demonstrated no significant difference in all-cause mortality between patients with PTC younger than age 45 with and without positive lymph nodes. For patients age 45 and older with PTC, however, mortality was 46% greater in patients with lymphatic metastases compared with those without. Lymphatic metastases in patients with follicular cancers were significantly associated with increased mortality in patients older (HR 11.23) and younger (HR 2.86) than 45 years. A single institution series of 700 patients with DTC analyzing disease-specific mortality also reports a statistically significant risk ratio of 2.6 for patients with nodal metastases compared with those without. A study of papillary microcarcinomas <1 cm in size noted a statistically significant effect on survival for lateral but not central compartment lymph node metastases. Although a mortality risk is not uniformly identified in every series, high-quality observational data strongly suggest lower long-term survival rates in DTC patients with lymphatic metastases.
Lymphatic Metastases and DTC Staging
Historically, nodal status has been conspicuously absent from staging systems for DTC, primarily because of lack of data implicating nodal status as a negative prognostic indicator. Several such systems, including AGES, AMES, MACIS, and the European Organization for Research and Treatment of Cancer (EORTC) system, do not include an assessment of lymph node status, yet are useful predictors of survival. In 1987, the American Joint Committee on Cancer and International Union Against Cancer adopted a TNM classification for DTC with separate staging criteria for patients younger and older than 45 years ( Table 3 ). For younger patients, stage is based entirely on the presence or absence of distant metastases. For older patients, nodal involvement equates to stage IIIb, with distant metastases stage IV. Several retrospective studies have demonstrated a correlation between TNM stage and mortality in thyroid cancer, with independent validation of the prognostic value of the regional lymph node or N classification.
| Primary Tumor (T) Note: All categories may be subdivided: (a) solitary tumor, (b) multifocal tumor (the largest determines the classification). | |||
| TX | Primary T cannot be assessed | ||
| T0 | No evidence of primary T | ||
| T1 | T < 2 cm in greatest dimension limited to the thyroid | ||
| T2 | T > 2 cm but not > 4 cm in greatest dimension limited to the thyroid | ||
| T3 | T > 4 cm in greatest dimension limited to the thyroid or any T with minimal extrathyroid ext (e.g., ext. to sternothyroid muscle or perithyroid soft tissues) | ||
| T4a | T of any size extending beyond the thyroid capsule to invade subcutaneous soft tissues, larynx, trachea, esophagus, or recurrent laryngeal nerve | ||
| T4b | T invades prevertebral fascia or encases carotid artery or mediastinal vessels | ||
| All anaplastic carcinomas are considered T4 tumors. | |||
| T4a | Intrathyroidal anaplastic carcinoma – surgically resectable. | ||
| T4b | Extrathyroidal anaplastic carcinoma – surgically unresectable. | ||
| Regional Lymph Nodes (N) | |||
| Regional lymph nodes are the central compartment, lateral cervical, and upper mediastinal lymph nodes. | |||
| NX | Regional lymph nodes cannot be assessed. | ||
| N0 | No regional lymph node metastasis | ||
| N1 | Regional lymph node metastasis | ||
| N1a | Metastasis to Level VI (pretracheal, paratracheal, and prelaryngeal/Delphian lymph nodes) | ||
| N1b | Metastasis to unilateral, bilateral, or contralateral cervical or superior mediastinal lymph nodes | ||
| Distant Metastasis (M) | |||
| MX | Distant metastasis cannot be assessed | ||
| M0 | No distant metastasis | ||
| M1 | Distant metastasis | ||
| STAGE GROUPING | |||
| Separate stage groupings are recommended for papillary or follicular, medullary, and anaplastic (undifferentiated) carcinoma. | |||
| Papillary or Follicular UNDER 45 YEARS | |||
| Stage I | Any T | Any N | M0 |
| Stage II | Any T | Any N | M1 |
| Papillary or Folicular 45 YEARS AND OLDER | |||
| Stage I | T1 | N0 | M0 |
| Stage II | T2 | N0 | M0 |
| Stage III | T3 | N0 | M0 |
| T1 | N1a | M0 | |
| T2 | N1a | M0 | |
| T3 | N1a | M0 | |
| Stage IVA | T4a | N0 | M0 |
| T4a | N1a | M0 | |
| T1 | N1b | M0 | |
| T2 | N1b | M0 | |
| T3 | N1b | M0 | |
| T4a | N1b | M0 | |
| Stage IVB | T4b | Any N | M0 |
| Stage IVC | Any T | Any N | M1 |
| Medullary Carcinoma | |||
| Stage I | T1 | N0 | M0 |
| Stage II | T2 | N0 | M0 |
| Stage III | T3 | N0 | M0 |
| T1 | N1a | M0 | |
| T2 | N1a | M0 | |
| T3 | N1a | M0 | |
| Stage IVA | T4a | N0 | M0 |
| T4a | N1a | M0 | |
| T1 | N1b | M0 | |
| T2 | N1b | M0 | |
| T3 | N1b | M0 | |
| T4a | N1b | M0 | |
| Stage IVB | T4b | Any N | M0 |
| Stage IVC | Any T | Any N | M1 |
| Anaplastic Carcinoma | |||
| All anaplastic carcinomas are considered Stage IV | |||
| Stage IVA | T4a | Any N | M0 |
| Stage IVB | T4b | Any N | M0 |
| Stage IVC | Any T | Any N | M1 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


