Fig. 1
Keloid scarring on the deltoid area following vaccination. A patient who may have valid reasons for avoiding a visible neck scar
Patient Selection for Robotic-Assisted Parathyroidectomy
As with all surgical operations, careful patient selection is paramount to the successful implementation of RAP. Patients should be carefully evaluated preoperatively and RAP only offered to those considered suitable. Multidisciplinary management with an endocrinologist is essential. The diagnosis of pHPT needs to be confirmed by demonstrating a raised serum calcium and parathyroid hormone (PTH). Vitamin D deficiency and Familial Hypocalciuric Hypercalcemia (FHH) need to be excluded by measuring serum vitamin D levels and 24-h urine calcium:creatinine clearance ratios respectively as these do not require surgical intervention [2].
There are parathyroid specific as well as generic considerations for RAP. With regard to the parathyroid, the indications for RAP are the same as for any targeted parathyroidectomy approach. Hence, RAP should only be offered to patients who have pHPT with a preoperatively localized adenoma. The authors advocate triple modality concordance as a prerequisite using ultrasonography, sestamibi scintigraphy and single-photon emission computed tomography (SPECT-CT) to minimize the risk of failure. However, it is likely that dual modality concordance (with ultrasonography and sestamibi scintigraphy) is just as adequate. The accuracy of localizing a single adenoma is reported to be 94–99 % with this modality [2].
There is no limitation to the size of the adenoma, and contrary to thyroid nodules that can reach a very large size, parathyroid adenomas are usually relatively small. RAP should not be offered to patients where there is suspicion of malignant disease, a coexistent large goiter ipsilaterally, history of previous neck surgery or irradiation and to those with a large body habitus. Relative contraindications to RAP include ipsilateral degenerative shoulder pathology or significant co-morbidity placing them in an American Society of Anesthesiologists (ASA) category greater than 2. The contraindications to RAP are summarized in Table 1.
Table 1
Contraindications to robotic-assisted parathy-roidectomy
Contraindications to robotic-assisted parathyroidectomy |
|---|
• Large goiter ipsilaterally |
• Suspicion of parathyroid carcinoma |
• Previous neck surgery |
• History of neck irradiation |
• A large body habitus (BMI > 30) |
• Degenerative shoulder pathology ipsilaterally |
• Significant co-morbidity (ASA > 2) |
The location of the parathyroid adenoma (including extracervical—ectopic location) is not a contraindication and a robotic-assisted thoracoscopic approach has been described to remove ectopic parathyroid adenoma in the mediastinum [20–23]. This approach is beyond the scope of the chapter.
The ideal RAP patient would be a slim female with a preoperatively localized parathyroid adenoma showing concordance on at least 2 imaging modalities.
Consent for Robotic-Assisted Parathyroidectomy
As with all surgical operations, informed consent is essential and should be undertaken by the attending surgeon. The literature supports that RAP is as safe as conventional parathyroidectomy [2, 3, 16, 17, 24, 25]. The risks associated with RAP are the same as for conventional parathyroidectomy with regard to the recurrent laryngeal nerve, infection, hematoma and hypoparathyroidism. Despite the anaerobic nature of the axilla, the literature does not support an increased infection rate with RAP compared to cervical parathyroidectomy [2, 3, 16, 17, 24, 25]. This “shifting” of the incision does however significantly prolong the operative time as a long subcutaneous flap must be raised to reach the neck and this should be explained to the patient. This may be associated with sensory changes of the overlying skin and higher pain scores and dysesthesia over the area of subcutaneous dissection. These symptoms are usually temporary [2, 16].
The two different approaches should be explained during the consent process. In general, the transaxillary incision is recommended for females because of breast concerns. For males, an infraclavicular incision can be used instead. The approach needs to be decided in conjunction with the patient at the time of obtaining their informed consent.
In the event of a post-operative hematoma, this is less likely to lead to airway obstruction because the potential space for the hematoma to disseminate is so capacious compared to cervical parathyroidectomy.
Another important point that the patient needs to be made aware of is the potential complication of developing a brachial plexus neurapraxia. The postulated mechanism is a traction injury when the ipsilateral arm is raised to reduce the distance between the axilla and anterior neck [26, 27]. This stretch injury is rare and can be prevented by adjusting the position of the ipsilateral arm with the patient awake to assess for comfort [28]. The back of the patient’s hand is positioned so that it is touching the central portion of the forehead. This is known as the “extended salute” position.
Robotic-Assisted Parathyroidectomy: Surgical Technique
Approaches for RAP
There are two distinct approaches for RAP: (1) the transaxillary approach [2, 16, 17, 24, 25] and (2) the infraclavicular approach [3]. The transaxillary incision is preferred for females due to concerns regarding breast scar cosmesis. For male and selected female patients, a 3 cm infraclavicular incision can be used instead as this minimizes the area of subcutaneous dissection when raising the flap. The disadvantage of the infraclavicular approach is that it requires two additional 5 mm trocar skin incisions. These are made high in the anterior axillary line and skin–areolar junction of the nipple whereas the axillary approach requires only one 6 cm incision. Both approaches are described in detail below.
Operative Set-up
1. Preoperative Considerations
Team work is essential in the preoperative preparation of the patient and setting up of the operating room (OR). The ipsilateral arm to the parathyroid adenoma must be free of identification bracelets, lines, blood pressure cuffs or ECG leads.
Transaxillary Approach RAP
For the transaxillary approach it is important to position the patient’s ipsilateral arm when they are awake in order to ensure comfort and thus minimize the risk of traction on the brachial plexus with subsequent neurapraxia. The arm position involves the back of the patient’s hand touching the central portion of the forehead, in an “extended salute” position (Fig. 2). A 5–6 cm axillary incision is also marked at this point as in our experience this is the optimal way to plan where to place the incision to prevent subsequent migration (Fig. 3). The incision may need to be extended superiorly in a curvilinear fashion so that it sits in a natural crease which reduces tension and a tendency towards hypertrophic and pigmented scarring (Fig. 4).



Fig. 2
The “extended salute” position for transaxillary robotic-assisted parathyroidectomy. By adjusting the position of the ipsilateral arm with the patient awake to assess for comfort, the risk of traction injury to the brachial plexus is prevented. Doing so and marking the incision immediately prior to surgery constitute vital components of preoperative planning
Fig. 3
Surgical position for left transaxillary robotic-assisted parathyroidectomy (laterality pre-marked with arrow). The 5–6 cm axillary incision has been pre-marked and re-checked once the patient is positioned on the operating table as in our experience this is the optimal way to plan where to place the incision to prevent subsequent migration. C cricoid cartilage, S suprasternal notch, A1 superior axillary, AM mid-axillary, A2 inferior axillary points of incision
Fig. 4
Axillary incision at the end of right transaxillary robotic-assisted parathyroidectomy. The incision has been extended superiorly in a curvilinear fashion so that it sits in a natural crease. This reduces tension and a tendency towards hypertrophic and pigmented scarring
Infraclavicular Approach RAP
If an infraclavicular approach has been chosen (incision usually 3 cm in length), this is also marked at this stage as are the sites of insertion for the two trocars in the ipsilateral anterior axillary line and periareolar region, respectively. The infraclavicular approach is particularly useful in the muscular male with a hirsute anterior chest wall. With experience and correct planning the incision heals well and becomes almost invisible (Fig. 5).

Fig. 5
Patient 4 weeks after right robotic-assisted parathyroidectomy via an infraclavicular approach. The 3 cm infraclavicular incision is barely visible as are the ports of entry for the trocars. With experience and correct planning the incisions heal well and become almost invisible. This approach is particularly useful in the muscular male with a hirsute anterior chest wall
At this stage, the anesthesiologist intubates the patient and ventilates them via a transoral endotracheal tube with electrodes (NIM EMG Endotracheal Tube, Medtronic, Inc, Jacksonville, FL). The correct positioning of the NIM EMG endotracheal tube with the electrodes at the level of the glottis is confirmed by direct laryngoscopy. Visualization of the electromyographic waveform on the nerve integrity monitor (NIM) following insertion of the stimulator and earth leads serves as additional confirmation. An extended tip of the NIM must be available due to the long distance between the incision (transaxillary or infraclavicular) and neck [17]. At induction, the patient is routinely administered intravenously 1.2 g co-amoxiclav and 4 mg dexamethasone.
2. Operating Room Set-up
Prior to transfer of the patient to the operating table it is important that all three components of the da Vinci robotic system are appropriately positioned. The cart is placed on the opposite side of the operating table as shown in Fig. 6. The cart is draped and correctly positioned before the patient is moved onto the operating table in preparation for docking. The vision cart is placed to one side of the patient so that the assistant surgeon, scrub nurse and anesthesiologist all have an unobstructed view. The console surgeon can be positioned anywhere in the operating room or even in a remote area (telerobotic surgery). The standard OR configuration used is illustrated in Fig. 7.

Fig. 6
The patient cart component of the robotic surgical system is covered with sterile drapes and comes in at right angles on the opposite side of the table to the parathyroid adenoma in question
Fig. 7
Operating room configuration for right robotic-assisted parathyroidectomy
Contrary to conventional parathyroid surgery, a shoulder roll is not placed under the shoulders as this has a tendency to hyper-extend the neck and move the superior pole of the thyroid gland away from the robotic instruments. Instead, a pillow is placed under the patient’s head and shoulders to provide adequate and comfortable support in a subtle “sniffing the morning air” position. The head of the table is then dropped by about 20° to widen the angle between the arm and the chest.
Transaxillary Approach RAP
For the transaxillary approach, a special arm rest supports the arm which is abducted and flexed with the forearm being pronated so that the back of the hand rests on the central portion of the forehead. A Velcro coin is attached to the hand and forehead to maintain the position (Fig. 8). This position shortens the distance between the incision site and parathyroid adenoma by elevating and externally rotating the clavicle. This is a modification to Chung’s method for RAT where the arm is fully extended over the head. We advise against the fully extended arm position as this puts the brachial plexus at risk through traction. We have had no such problems since modifying Chung’s method of arm positioning.

Fig. 8
Transaxillary robotic-assisted parathyroidectomy: a special arm rest supports the arm which is abducted and flexed with the forearm being pronated so that the back of the hand rests on the central portion of the forehead. A Velcro coin is attached to the hand and forehead to maintain the position. This position shortens the distance between the incision site and parathyroid adenoma by elevating and externally rotating the clavicle
Infraclavicular Approach RAP
If the infraclavicular approach is used the ipsilateral arm is maintained in the neutral position. Once completed, the incision site is infiltrated with 10 ml of 1 % lidocaine and 1:200,000 epinephrine. Skin preparation and draping then take place.
The Operation
A. Preparation of the Robotic Field
Transaxillary Approach RAP
Following the axillary incision, a subcutaneous flap is raised anterior to the clavipectoral fascia. The superior and inferior points of the axillary incision are extended to the thyroid cartilage and sternal notch, respectively. The resulting shape of the flap is that of a trapezoid.
In taller patients, if the distance from the axilla to the sternal notch exceeds the limit of the instruments, the robot can be docked in earlier to perform the last (most distal) part of the subcutaneous flap raising. The technique for entering the neck is identical to the one described below but is performed robotically. This modification expands the range of patients to whom transaxillary RAP can be offered [16].
Infraclavicular Approach RAP
If the infraclavicular approach is used, then the flap is raised from the infraclavicular incision to the neck and the two trocars tunneled through small incisions made in the ipsilateral anterior axillary line or periareolar incision for the inferior 5 mm trocar.
Once the subcutaneous flap is raised, dissection is continued above the pectoralis major and over the clavicle. At this point, the sternal and clavicular heads of the sternocleidomastoid muscle are identified and the neck entered through the natural dehiscence between the two. The surgical planes are then developed as in a standard parathyroidectomy. The internal jugular vein, common carotid artery and ipsilateral omohyoid and sternohyoid muscles are exposed. The flap and strap muscles are retracted by a table-mounted self-retaining retractor (Chung, Kuppersmith, Modena or Imperial) to create sufficient working space to access the thyroid lobe laterally. No gas insufflation is required for either transaxillary or infraclavicular RAP. At this point, the da Vinci robot is docked.
B. Docking
The cart is docked at right angles to the operating table.
Transaxillary Approach RAP
All three robotic arms can be placed through the single axillary incision. The 30° down 12 mm stereoscopic endoscope is placed at an angle of 220° and is inserted low laterally extending high and upwards medially towards the thyroid gland. The 4th arm can then be placed under the endoscope which is used to contra-laterally retract the thyroid lobe. Finally, the 1st and 3rd arms are positioned which carry the instruments for dissection and hemostasis. The 4th assistant arm holds the 8 mm Prograsp, while 1st and 3rd arms have a combination of 5 mm Maryland, Debakey and Harmonic shears.
Infraclavicular Approach RAP
If the infraclavicular approach is used, a 30° down 12 mm stereoscopic endoscope is introduced into the operative field via the 3 cm infraclavicular incision. Two 5 mm robotic instruments are used. These are the Maryland and Debakey forceps which are inserted through the superior and periareolar trocars respectively until they come into view in the operative field.
C. Robotic Surgery
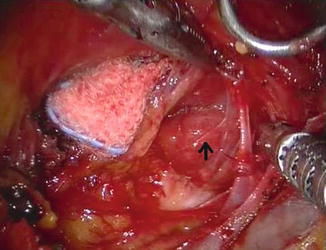
The robotic dissection begins with exposure of the ipsilateral inferior thyroid pole, trachea, recurrent laryngeal nerve (RLN) and parathyroid adenoma (Figs. 9 and 10). The RLN is stimulated routinely (NIM nerve integrity monitor; Medtronic, Inc). Once the adenoma and its vascular pedicle are delineated, the Debakey dissector is replaced with the 5 mm Harmonic curved shears (Ethicon Endo-Surgery, Inc, Johnson & Johnson, Cincinnati, OH) and the pedicle sealed and divided allowing resection of the adenoma. As with all energy-based hemostatic devices, great care should be taken when using this instrument close to the RLN [29]. We do not routinely use intraoperative quick PTH (iQPTH) monitoring [3].
 < div class='tao-gold-member'>
< div class='tao-gold-member'>




Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
