CHAPTER 52 Surgery of the lacrimal system

Background
Lacrimal surgery existed in the Middle Ages for the treatment of dacryocystitis from a blocked nasolacrimal duct, albeit restricted to crude external drainage of abscess and extirpation of the lacrimal sac. It is not until the late 18th century that more modern techniques for draining the tear sac into the nose were introduced and it took some years for such dacryocystorhinostomy (DCR) surgery to be widely available (Fig. 52.1).
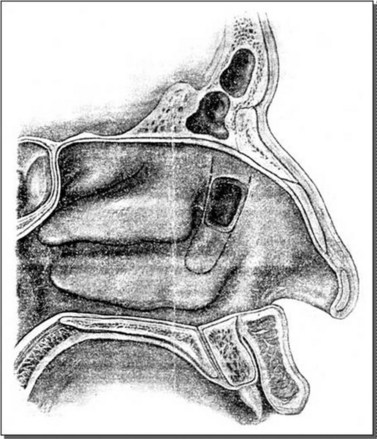
Fig. 52.1 Diagram of endonasal DCR by West.
West JM, A window resection in the nasal duct in cases of stenosis. Trans Am Ophthalmol Soc 1910;12:654–8. Kept at Royal Society of Medicine in London.
Definitions
There are various abbreviations and different operations.
Table 52.1 Etymology of the term Dacryocystorhinostomy
| 4 parts: dacro – cysto – rhino – stomy | ||
|---|---|---|
| Ancient Greek | Transliteration | Translation |
 | dakruon | tear |
 | kustis | bladder, sac |
 | rhis | nose |
 | stoma | mouth |
History of modern DCR
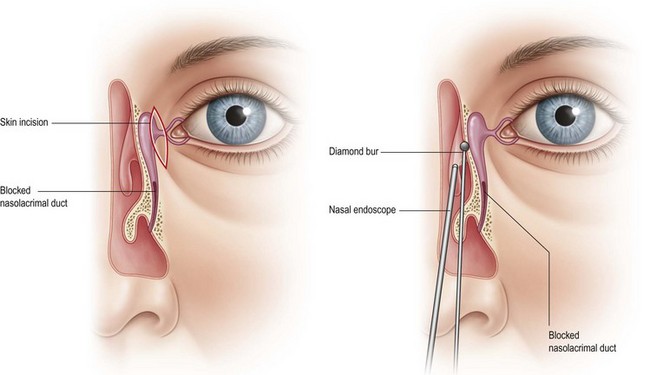
Endonasal approach lacrimal surgery has developed further in the last 15 years using endoscopic techniques and visualization with a Hopkins rigid nasal endoscope (Fig. 52.3). Endoscopic endonasal dacryocystorhinostomy (EE-DCR) is a primary treatment for nasolacrimal duct obstruction with a number of advantages compared with the traditional external approach. These advantages include avoidance of a cutaneous scar, direct visualization of nasal anatomy, and preservation of medial canthal tendon and pump function. The success rate for primary endonasal DCR surgery is comparable to the external approach.
Normal anatomy
Tear drainage
The tears normally drain through the puncta to the nose where they can be seen in the inferior meatus (Fig. 52.4).
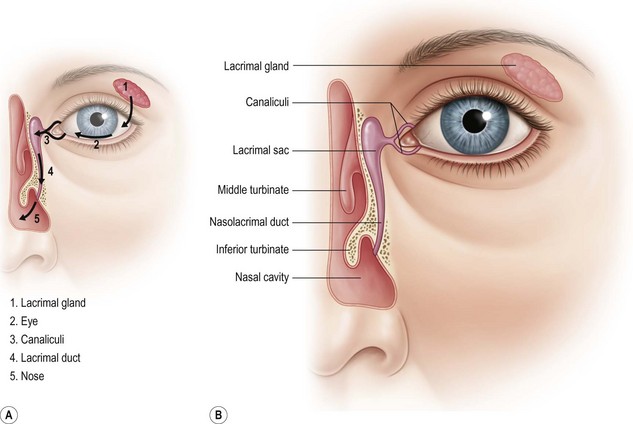
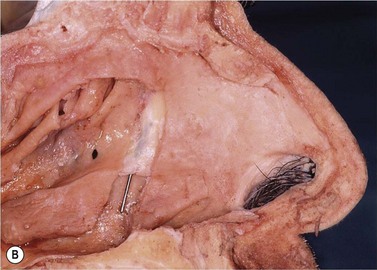
Fig. 52.4 (A) Normal tear drainage. (B) Anatomy of lacrimal system.
Courtesy of Santiago Ortiz-Perez.
Nasal anatomy
Soft tissue and bones of the lateral nasal wall
The main soft tissue structures of the lateral nasal wall are:



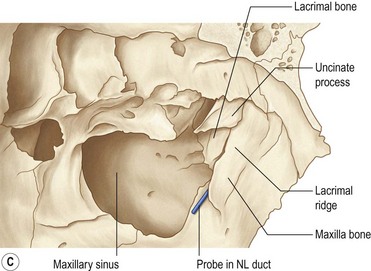
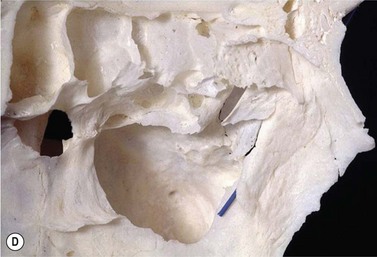
The main bones of the lateral nasal wall are (Fig. 52.6):

Etiology and assessment of watering eye
Blocked nasolacrimal duct in adults
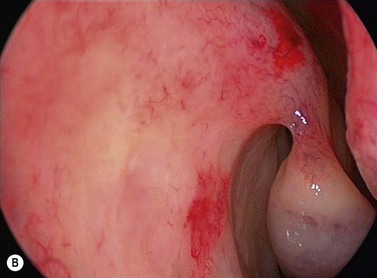
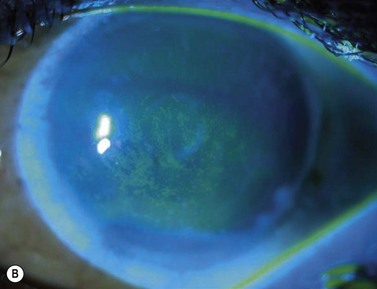
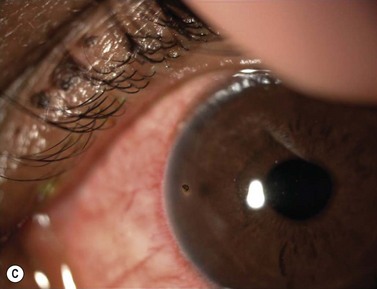
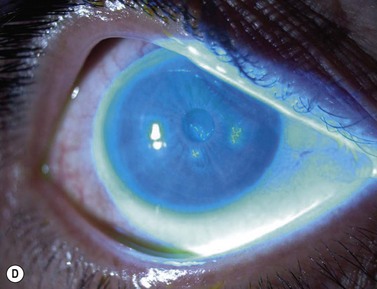
The causes of a watering eye include hypersecretion and epiphora. Causes of hypersecretion (conjunctivitis, keratitis, corneal foreign body, etc.) should be excluded (Fig. 52.7A–D). Surgery of the lacrimal system is for epiphora, which is an outflow problem cause by a stenosis or obstruction of the lacrimal excretory system or very poor functional drainage, as for instance may occur in facial nerve paralysis.

The periorbital area should be examined and a mucocoele, dacyocystitis (Fig. 52.8), and fistula from the lacrimal sac should be excluded. Eyelid position, particularly punctual apposition to the globe, should also be recorded.


Canaliculitis is an often missed yet relatively common condition (Fig. 52.9). It is a simple diagnosis because the small swelling is medial to the punctum, which commonly has with some yellow discharge. It can be chronic and partially responsive to topical medication, with surgery the definitive treatment.





