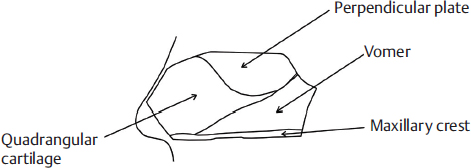
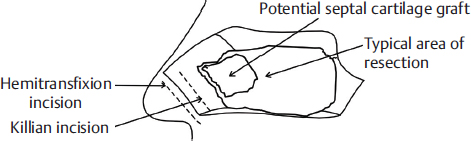
14 Surgery of the Inferior Turbinates and Septum: Principles and Techniques Septal surgery is one of the most common procedures performed by a rhinologist. Septal abnormalities and turbinate hypertrophy can often prohibit the introduction of endoscopic instruments, and limit good visualization during surgical management of sinus and skull base pathology. Septal surgery is also often required to achieve other important objectives: maximizing nasal tip and dorsal stability, establishing an adequate and long-lasting airway for the patient, and removing any sinus outflow obstructions. While conventional closed septoplasty is a standard surgical approach for many otolaryngologists, conservative and endoscopic techniques are becoming more prominent. This chapter reviews techniques for both approaches as well as turbinate reduction, which commonly accompanies septal deviation surgery. The nasal septum is the vertical midline structure that extends posteriorly from the columella and divides the nose into roughly symmetric halves. It consists of bone, cartilage, and soft tissue (Fig. 14.1). The bony components include the perpendicular plate of the ethmoid bone (PPE), the vomer, the perpendicular plate of the palatine bone, and the palatine extension of the maxilla.1 The latter two components together are commonly known as the maxillary crest. The cartilaginous septum sits anterior to the vomer and PPE, and is roughly diamond-shaped or quadrangular. A sphenoid extension of cartilage extends between the vomer and PPE up toward the rostrum. The septal cartilage has dense fibrous attachments to the nasal bones and PPE superiorly, the vomer posteroinferiorly, and the palatine process and nasal spine of the maxilla bone caudally. The bony and cartilaginous septal floor is anatomically stabilized in a groove of the maxillary crest. The inferior turbinates are paired structures consisting of bone and soft tissue that run the length of the inferior meatus from the pyriform aperture anteriorly often to the choana posteriorly. The inferior turbinate bone is a thin, curved bone that articulates with the maxilla at the lateral nasal wall. The nasal septum and inferior turbinates are covered with pseudostratified ciliated (respiratory) epithelium with numerous mucous-producing goblet cells. Beneath the epithelium is the lamina propria, which is rich with seromucinous glands and cavernous vascular tissue with large venous sinusoids. The septal blood flow is supplied by branches from the ethmoidal, sphenopalatine, greater palatine, and labial arteries. Innervation of the septum is from all three divisions of the trigeminal nerve. Knowledge of each branch is important for proper injection of local anesthetics and vasoconstrictors before surgery.1 Figure 14.1 Nasal septal anatomy. Nasal airway obstruction remains the most common indication for surgery of the nasal septum and turbinates. Turbinate and rarely septal mucosal abnormalities can result in turbulent nonlamellar nasal airflow and the subjective sensation of nasal obstruction. Mucosa blood flow cycles can be altered by an inflammatory or infectious process. This can cause inflammatory cell infiltration of the lamina propria, reactive engorgement of the venous sinusoids, and subepithelial edema. Examples of such processes include infectious rhinosinusitis and allergic rhinitis. Secondary changes to the lymphatic and venous drainage, and to the connective tissue within the lamina propria after prolonged inflammation, lead to more permanent hypertrophy of these structures. This renders more resistance to topical decongestants and anti-inflammatory medications such as steroids. Nasal airflow and/or sinus outflow tracts can also be disrupted by anatomic abnormalities such as septal deviation, spur, fracture, or dislocation from the maxillary crest. These may be caused by former nasal trauma, previous surgery, or congenital factors. When nasal airway obstruction persists despite maximal medical management, such as nasal steroids and topical antihistamines, surgical treatment is indicated.2,3 Septoplasty may also be indicated for a deviated septum if the patient has epistaxis, intolerance to continuous positive airway pressure (CPAP) treatment, osteomeatal complex obstruction, or access obstruction for sinonasal procedures unrelated to the septum. A proper history and physical examination with nasal fiberoptic evaluation is used to rule out other potential causes of nasal obstruction that may need to be addressed.2 Allergic rhinitis, rhinitis medicamentosum, polyps, neoplasms, concha bullosa, adenoid hypertrophy, choanal and pyriform stenosis, severe nasal dorsal deformity, lateral nasal wall collapse, and poor tip support should be properly diagnosed and managed. A history of obstructive sleep apnea (OSA) and CPAP intolerance should prompt a thorough evaluation of the entire upper airway. The region of septal deflection should also be noted during the examination as this will guide proper surgical planning and technique. A more caudal deviation may prompt a traditional closed approach to the septum, for example, while an isolated more posterior deviation or spur may be better addressed endoscopically.4,5 Septal surgery can be complicated by congenital or traumatic pathology, former attempts at septoplasty or septectomy, preexisting septal perforation, or other obstructing intranasal pathology such as polyps. Complex cases should prompt an open and honest discussion with the patient concerning the higher risk for complications and reasonable expectations. Although not always necessary, CT imaging may be useful to provide detailed anatomy of the septum and further evaluate concurrent sinonasal disease, such as chronic rhinosinusitis, concha bullosa, congenital narrowing of the pyriform or choana, nasal polyposis, or a neoplastic process. Patients should also be informed preoperatively about what to expect after surgery and the common and most severe complications that can occur. Septoplasty can be performed with appropriately administered local anesthesia and sedation, however, the procedure is usually performed under general anesthesia. The most important surgical preparations in either situation are the use of a topical decongestant (oxymetazoline, neosynephrine, or 4% cocaine solution) and submucoperichondrial injection of a local anesthetic mixture containing epinephrine (1:100,000 being the most common concentration). Under headlight illumination, a #15 scalpel is used to make either a hemitransfixion incision at the caudal edge of septal cartilage or a Killian incision just rostral to it (Fig. 14.2); these incisions allow approach to the septum to remove deviations and spurs, or when septal cartilage is needed for grafting purposes. Using a scraping maneuver (e.g., with a scalpel, freer, Cottle, or iris scissors), the submucoperichondrial plane is identified as a relatively avascular plane between glistening perichondrium and the more opaque, grainy-textured surface of septal cartilage. Planes should easily separate in this area with sharp then blunt elevation. Establishing the correct plane helps minimize blood loss and prevent septal tears. A nasal speculum is placed in the incision with intermittent use of a Frazier suction to improve visualization. Figure 14.2 Septoplasty incisions.
Anatomy
Preoperative Patient Evaluation
Surgical Technique
Septoplasty
Traditional Closed Headlight Approach
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


