25
Surgery in Bell’s Palsy and In Traumatic Facial Paralysis
■ Bell’s Palsy
The facial weakness of Bell’s palsy is usually unilateral, and most often, the symptoms appear in an acute form. The degree of initial facial weakness can vary from slight weakness of facial motion to complete paralysis (House-Brackmann1 grade VI) (Table 25–1). It can also progress from one level to the next in the course of a day or two. Sometimes the paralysis is recurrent. When it is ipsilaterally recurrent, a diligent search for a tumor along the entire course of the nerve must be made with detailed imaging. Contralateral recurrent paralysis is another form of Bell’s palsy. The cause of Bell’s palsyhas long been held to be idiopathic, but now, based on clinical, histopathologic, experimental, imaging, and therapeutic evidence, an infection of the nerve with herpes simplex type 1 virus is the accepted etiology.2–6 The resultant inflammation and edema of the nerve cause neural compression at the meatal foramen. This is the narrowest, medialmost part of the fallopian canal, located at the fundus of the internal auditory canal. Fisch7 termed this narrowed segment of the canal the bottle neck. Clinically, although two patients may present with an identical severity of paralysis, recovery in one may be excellent, and in the other it could be poor and complicated by disfiguring synkinesis. Can we, as neurotologists, predict the outcome and know whether medical or surgical treatment would be most appropriate? The answer to both questions is yes, within limits, provided the patient is willing to undergo serial electrophysiological tests. Both the selection of the most appropriate test and the interpretation of the test results will be facilitated by an understanding of facial nerve anatomy and the pathophysiology of nerve degeneration and regeneration.
The facial nerve is a composite nerve containing ~10,000 nerve fibers, of which 7000 are branchial motor, and these innervate the musculature derived from the second branchial arch. The majority of these muscles are the muscles of facial expression. The remaining nerve fibers are afferent taste fibers from the anterior two thirds of the tongue (cell bodies in the geniculate ganglion) and efferent parasympathetic motor fibers to the lacrimal, nasal, submandibular, and sublingual glands.8 The structure of each branchial motor axon is similar to any peripheral nerve except that the size is different. The axoplasm is surrounded by a myelin sheath, and these myelinated fibers are encased in a connective tissue tubule called endoneurium (Fig. 25–1). In peripheral nerves, groups of such axons are surrounded by concentric sleeves of flattened polygonal cells called perineurium. Each such collection of axons enclosed by perineurium, is called a fascicle. Peripheral nerves are made up of groups of fascicles, which in turn are held together by a condensation of loose areolar connective tissue called epineurium (Fig. 25–2). However, the structure of the facial nerve has been shown to be different from peripheral nerves in that in the seventh nerve there is only a single fascicle in most of its intratemporal course.9, 10 According to Sunderland’s classification (Table 25–2), in first-degree paralysis, there is a physiological block to nerve impulse transmission at the site of the injury (Fig. 25–3). The structure of the nerve at the site of the injury, as well as proximal and distal to it, is normal. It is for this reason that, though the face is paralyzed, electrical stimulation of the distal extratemporal segment elicits a response, equal to that obtained on the normal side. A Sunderland second-degree injury may develop if the degree of compression at the meatal foramen continues to increase. In such a case the axoplasm and myelin sheath are destroyed, but the endoneural tubes are unaffected (Fig. 25–4). If only a minority of axons suffer this degree of injury and the rest just have a conduction block, as already described, electrical stimulation of the distal extratemporal facial nerve will elicit a response that would be only moderately less than the response obtained on the normal side. It should be noted that in such patients, because the endoneural tubules are intact, regenerating fibers are able to reach their appropriate destinations. Thus functional recovery occurs without synkinesis. In a majority of patients, the pathological process in Bell’s palsy does not progress beyond a Sunderland second-degree injury. This assumption is supported by Pietersen’s11 observation that 71% of untreated Bell’s palsy patients (in a cohort of 1011) recover without any sequelae. With continued increase in intraneural pressure, the equivalent of Sunderland’s third- and fourth-degree injury occurs in the distal nerve. In the facial nerve, because there is only one fascicle, the equivalent of a Sunderland grade III or IV injury is the destruction of a greater number of axons. The antegrade pathological changes that occur in a nerve damaged by a Sunderland grade III or greater injury is called Wallerian degeneration. These changes begin ~12 hours after the insult. The axoplasm is destroyed, and the myelin sheath disintegrates and is phagocytosed by activated macro-phages. The endoneurial tubes are destroyed, and the Schwann cells proliferate to form the bands of Büngner’s bands. These in turn strongly support axonal regeneration. Because the endoneural tubes are destroyed, there is no assurance that the regenerating fibers will reach their appropriate destinations. This is the reason that varying degrees of synkinesis are observed in patients with an injury greater than Sunder-land grade III. Wallerian degeneration is generally complete within 12 to 14 days postinjury. Regenerated axons have thinner myelin sheaths, and as a result the threshold for depolarization is increased and nerve conduction velocity is slowed.
Grade | Description | Characteristics |
|---|---|---|
I | Normal | Normal facial function in all areas |
II | Mild dysfunction | Gross: Slight weakness noticeable on close inspection; may have very slight synkinesis At rest: Normal symmetry and tone Motion: Forehead—moderate to good function; eye—complete closure with minimum effort; mouth—slight asymmetry |
III | Moderate dysfunction | Gross: Obvious but not disfiguring difference between two sides; noticeable but not severe synkinesis; contracture and/or hemifacial spasm At rest: Normal symmetry and tone Motion: Forehead—slight to moderate movement; eye—complete closure with effort; mouth—slightly weak with maximum effort |
IV | Moderately severe dysfunctio | Gross: Obvious weakness and/or disfiguring asymmetry At rest: Normal symmetry and tone Motion: Forehead—none; eye—incomplete closure; mouth—asymmetric with maximum effort |
V | Severe dysfunction | Gross: Only barely perceptible motion At rest: Asymmetry Motion: Forehead—none; eye—incomplete closure; mouth—slight movement |
VI | Total paralysis | No movement |
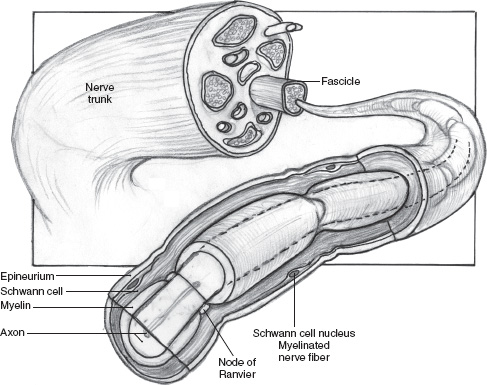
FIGURE 25-1 A myelinated nerve fiber.
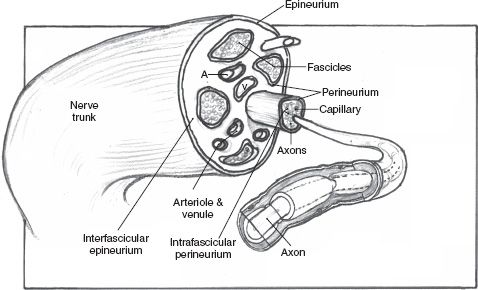
FIGURE 25-2 A multifascicular nerve. A, artery; V, vein.
Degree of Injury | Pathology |
|---|---|
First degree | Compression of axon without loss of structure |
Second degree | Destruction of axoplasm, myelin sheath; endoneurial tubes remain intact; recovery without synkinesis |
Third degree | Destruction of axoplasm, myelin sheath, and endoneurial tubes; recovery without synkinesis |
Fourth degree | Disruption of perineurium; recovery is poor because of scarring and loss of endoneurial tubes |
Fifth degree | Complete transection of nerve; no spontaneous recovery |
Retrograde changes in the nerve segment proximal to the site of the injury and in the corresponding cell body begin within 5 hours of the injury. The cytoplasm of the cell swells, the nucleus of the cell is pushed to an eccentric position, and the Nissl granules disappear. Wallerian degeneration in the proximal segment does not usually extend beyond the second node of Ranvier. With stretch injuries of the nerve, intraneural fibrosis is often quite prominent, and it becomes an impediment to nerve regeneration.12
The two electrophysiological tests commonly used for evaluation of facial nerve function and for prognostication of return of function are electroneurography (ENoG) and electromyography (EMG). ENoG, popularized by Esslen 13 and Fisch,14 consists of stimulating the facial nerve percutaneously after its exit from the stylomastoid foramen. The resultant compound motor unit action potentials (CMUAPs) are recorded at the nasolabial fold (Fig. 25–5). The details of the stimulus parameters have been described by Gantz et al.15 Using maximal stimulation, the responses of the normal and paralyzed side are compared, and the response of the paralyzed side is expressed as a percentage of the normal side (Fig. 25–6). The peak-to-peak response on the paralyzed side represents the percentage of surviving and neuropraxic (Sunderland grade I) fibers. As the percentage of degenerated fibers within the nerve increases, the amplitude of the CMUAPs decreases when compared with the normal side. The chief value of the test is in prognostication of recovery of function. However, the test should be administered serially within the first 15 days of onset of paralysis. As shown in Fig. 25–7, if 60% of the fibers survive up to day 10 postonset of paralysis, the prognosis for recovery of function without synkinesis is excellent. To the patient, this kind of information, based on objective data, is most reassuring. For the surgeon too, this information is valuable as a guide to avoiding surgical decompression of the nerve. On the other hand, if by the sixth day postonset of paralysis there are only 5% or less surviving fibers (Fig. 25–7), then the prognosis for recovery of function is poor and most likely will be associated with synkinesis. In such patients, decompressive surgery is indicated. Because the site of the injury is at the meatal foramen and in the labyrinthine segment, an approach via a middle fossa craniotomy is most logical. Thus the time course of degeneration is important for purposes of both prognostication and management.
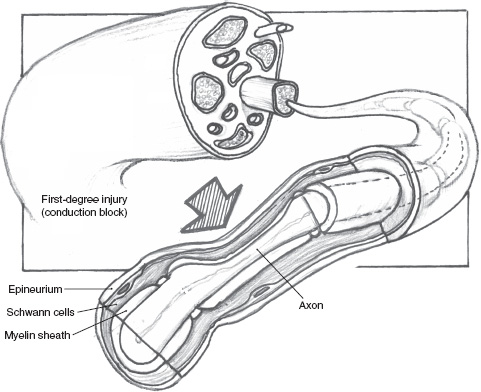
FIGURE 25-3 A Sunderland first-degree injury. Note that the myelin sheath and the endoneurium are intact, though the intraneural anatomy is distorted. The axoplasmic flow can occur in both directions.
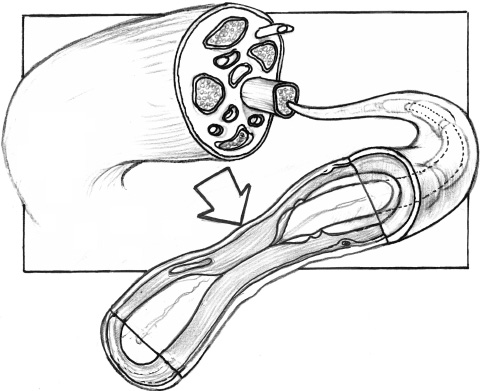
FIGURE 25-4 A Sunderland second-degree injury. The axoplasmic continuity is disturbed, and the myelin sheath is destroyed (arrow). However, the endoneurial tube is intact.
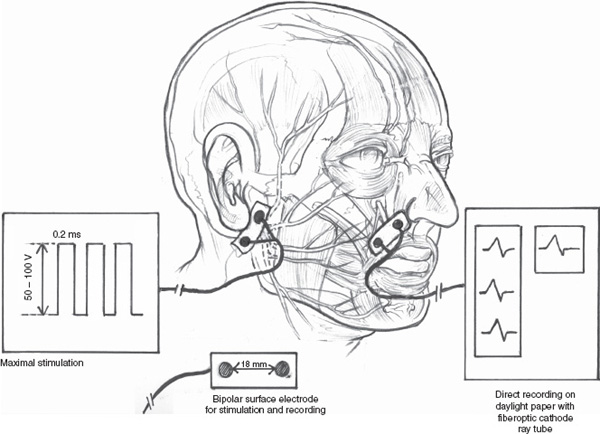
FIGURE 25-5 Diagrammatic representation of the setup for an electroneurographic study.
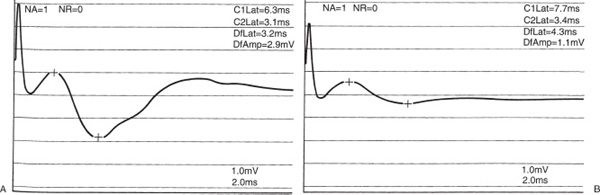
FIGURE 25-6 Comparison of the compound motor unit action potentials of the normal side (A) and the paralyzed side (B). (Used with permission from Nadol JB, McKenna MJ. Surgery of the Ear and Temporal Bone. 2nd ed. Philadelphia: Lippincott Williams & Wilkins; 2005:73.)
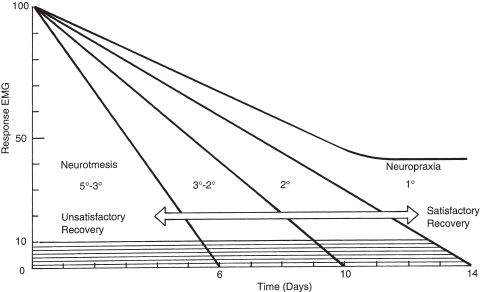
FIGURE 25-7 Graphic representation of serial compound motor unit action potential values recorded from day 1 to day 14 postonset of paralysis. (Used with permission from Nadol JB, McKenna MJ. Surgery of the Ear and Temporal Bone. 2nd ed. Philadelphia: Lippincott Williams & Wilkins; 2005:72.)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


