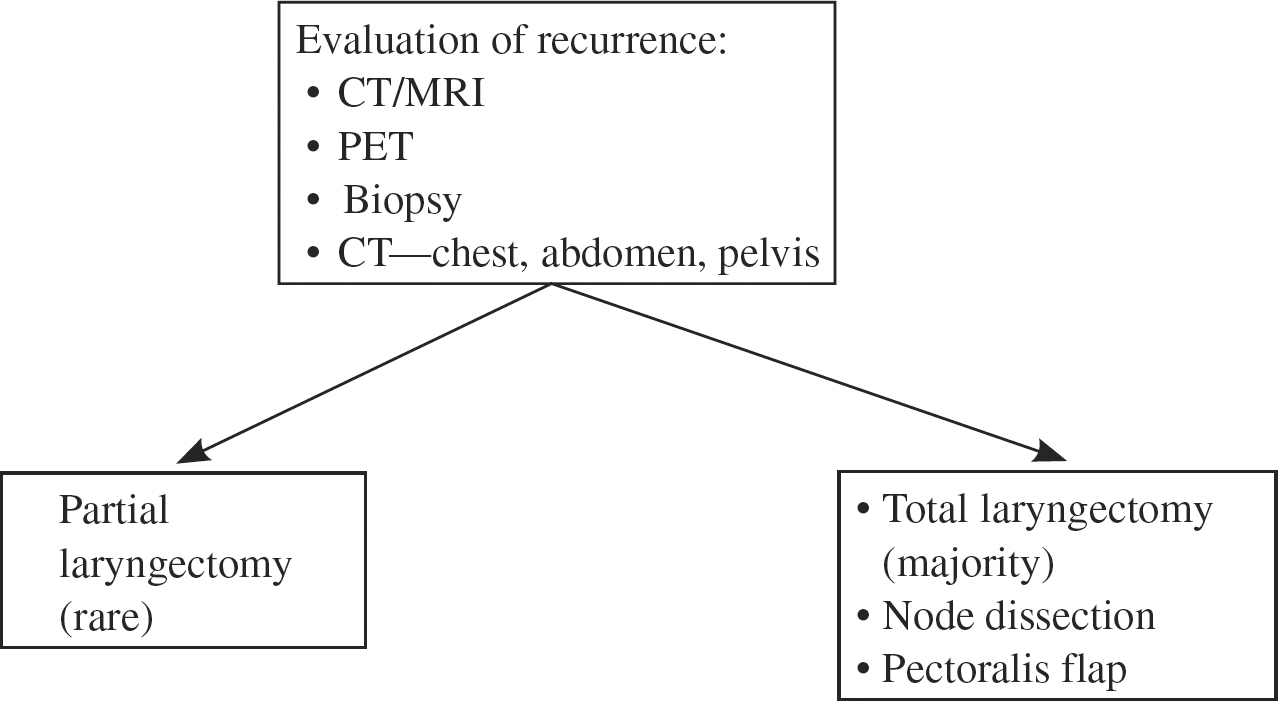
20 Surgery for Recurrence after Organ Preservation Management of Advanced Squamous Cell Cancers of the Larynx The pattern of care for the management of advanced laryngeal cancer has changed over the past 20 years. The traditional approach consisted of surgery followed by radiation therapy. All patients with glottic tumors and more than 70% of patients with supraglottic tumors underwent a total laryngectomy. The morbidity of a total laryngectomy, with its permanent tracheal stoma, is well recognized. Alternative therapies have been developed to preserve the laryngeal function. A major step toward the acceptance of alternative therapy came after the publication of the results from the Department of Veterans Affairs Laryngeal Cancer Study Group.1 In many centers, organ preservation approaches, either with radiation therapy alone,2,3 with radiation therapy combined with induction1 or concurrent chemotherapy,4 or with subtotal laryngectomy techniques,5,6 are now the preferred treatment modalities for the management of advanced laryngeal cancers. When extirpative surgery is not part of the initial treatment, the risk of local recurrence is greater than after surgery. The diagnosis and treatment of tumor persistence or recurrence after radiation therapy or after chemoradiation therapy can be challenging. In reality, the only recurrences that can be salvaged successfully are local recurrences. Approximately 30 to 50% of these can be salvaged. Patients with neck recurrences can rarely be successfully salvaged. Therefore, it has been my personal preference to perform a neck dissection, 6 to 8 weeks after completion of therapy, for all necks with less than a complete response, and for all necks stage N2 or higher on initial presentation, regardless of the response to therapy.7 The following discussion will be centered on the diagnosis and management of laryngeal recurrences. The determination of tumor persistence after therapy can be difficult. Some of the changes seen after therapy can mimic signs and symptoms of tumor persistence or recurrence. Mucosal and soft tissue abnormalities are expected after therapy for advanced laryngeal cancer. Mucositis and edema are almost always seen early after therapy. These changes tend to be worse and more prolonged after chemoradiotherapy than after radiation alone. Mucositis usually disappears within the first 2 months. Cartilage exposure and/or amputation of the superior aspect of the epiglottis are not unusual, especially after chemoradiation. This is accompanied by persistent pain that is aggravated on swallowing. Concentric scarring and stenosis of the oropharynx, larynx, and hypopharynx are sometimes seen as the mucositis resolves. Persistence of laryngeal edema after irradiation is seen in ~5% of patients.8 After chemoradiation the incidence has not been reported, but in my opinion it is present in the majority of patients. Late occurrence of edema is often a sign of tumor recurrence, but it can also be secondary to therapy and/or radionecrosis. The persistence of vocal cord immobility after treatment does not necessarily imply tumor persistence.8 Late onset of vocal cord immobility is somewhat more ominous. The detection of vocal cord immobility can be sometimes difficult in patients with significant supraglottic edema. Adequate documentation of the original location of the lesion is also useful in understanding some of the changes. Amputation of the area initially involved by the tumor is a common finding, especially at the level of the epiglottis. Residual ulceration after tumor necrosis can persist for a long time and in some patients forever. Tumor pain that is present before therapy often disappears during therapy. Pain induced by the treatment is almost always present within the first 2 or 3 weeks of irradiation. Persistence of pain for months after therapy is not unusual. Most often this pain is associated with persistent areas of ulceration and necrosis. Late onset of pain after therapy is highly suspicious for tumor recurrence, but it can also be secondary to radionecrosis. In conclusion, signs and symptoms observed after therapy can be significant even without tumor persistence or recurrence. Therefore, detection of tumor persistence and/or recurrence can be difficult and often delayed. Decision tree for the evaluation and management of recurrent laryngeal cancer after chemorodiation Imaging techniques are essential for the initial diagnosis and staging of laryngeal tumors in patients treated with organ preservation therapies. These techniques can also be used for the diagnosis of tumor recurrence. Hermans et al suggested that, in ~40% of patients, the routine use of computed tomography (CT) allowed for earlier detection of recurrence than clinical examination alone.9 However, anatomical studies such as CT and magnetic resonance imaging (MRI) are often difficult to interpret. Unless obvious changes such as tumor enhancement and/or necrosis are identified, the radiologist is often puzzled by the significant edematous changes noted after therapy.8 Few practitioners routinely order these diagnostic tests unless tumor recurrence or persistence is suggested by clinical findings. The recent addition of dynamic imaging techniques for the diagnosis of head and neck malignancies may be promising. Greven et al reported on 45 patients evaluated with positron emission tomography (PET) before and after irradiation.10 They tested patients as early as 1 month after therapy and concluded that a positive scan at any time post-therapy correlated with a high likelihood of tumor recurrence. They also noted that early negative scans were not accurate for the absence of disease: 7 of 25 patients with negative scans at 1 month eventually recurred. Terhaard et al reported on 75 patients, previously treated with irradiation, with suspected recurrent disease on clinical examination.11 PET scanning was positive in 36 of the 37 patients who eventually were proven to have recurrence. False-positive results were found in 7 of 38 patients who never recurred. The researchers concluded that a laryngoscopy and biopsy, with their inherent risk, could be avoided in patients with a negative PET. A positive PET warrants a biopsy. Routine imaging post-treatment is rarely performed. These tests are best reserved when tumor recurrence is suspected clinically. CT and MRI scanning are the techniques of choice. More data are needed before PET is recommended for routine evaluation of possible persistent disease.
Diagnosis
Clinical Evaluation
Imaging Techniques
Tissue Diagnosis
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Surgery for Recurrence after Organ Preservation Management of Advanced Squamous Cell Cancers of the Larynx
