Supracricoid Partial Laryngectomy
Ollivier Laccourreye
INTRODUCTION
The supracricoid partial laryngectomy (SCPL) is an important surgical option for patients with cancer of the larynx. The literature has demonstrated superior oncologic results, in terms of local control, when SCPLs are used for selected “early” endolaryngeal cancer (glottic, supraglottic, or transglottic in origin) when compared to transoral laser microsurgery, vertical partial laryngectomy, or radiation therapy as well as a valid alternative to chemoradiation protocols and total laryngectomy in the face of selected “intermediate-advanced” cancer of the larynx. Yet despite a wide resection of the endolaryngeal structures including both vocal cords and the thyroid cartilage, patients undergoing SCPLs maintain their own voice, normal swallowing, and no permanent tracheostomy.
Supracricoid partial laryngectomy includes three procedures: the cricohyoidopexy (CHP), cricohyoidoepiglottopexy (CHEP), and the tracheocricohyoidoepiglottopexy designed to resect selected glottic supraglottic and transglottic cancer while achieving phonation respiration and swallowing without the need for permanent tracheostomy, gastrostomy, or voice prosthesis. Currently more than 250 scientific reports from more than 15 countries document the worldwide diffusion and current use of the SCPL by numerous surgeons.
HISTORY
Patients who might be candidates for SCPL must be carefully evaluated for oncologic, functional, and wound-healing considerations. A patient with a large cancer with dyspnea or swallowing dysfunction is not an ideal candidate. Since all patients experience some temporary aspiration postoperatively, moderate to severe chronic obstructive pulmonary disease (COPD) should be considered a discrete contraindication. Formal pulmonary function testing is not usually needed. In fact, a commonly used assessment is the “step test.” If the patient has adequate pulmonary reserve to walk up two flights of stairs, then a favorable postoperative outcome is expected. While poor pulmonary function places patients at risk for postoperative pneumonia, other illnesses that affect the microcirculation such as lupus, diabetes mellitus, or history of radiation therapy place the patient at risk for wound-healing complications.
Patients who are candidates for SCPL must be carefully evaluated to determine their ability to undergo a rigorous postoperative rehabilitation. Thus, as part of the clinical history and discussion of postoperative recovery, the surgeon should provide realistic expectations for both voice outcomes and the rigor of postoperative rehabilitation.
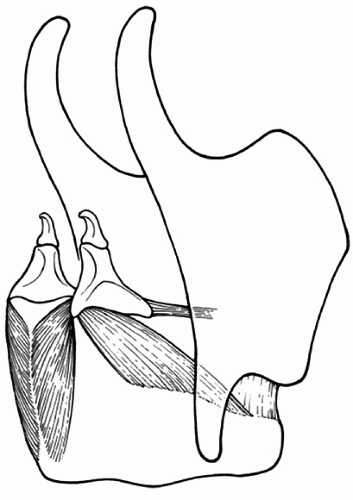 FIGURE 26.1 The SCPL hinges on the concept of the CA unit as the fundamental unit of laryngeal function. The CA unit is formed by the posterior and lateral CA muscles, the cricoid and arytenoid cartilages, and the nerves that supply sensory and motor function, the superior and inferior laryngeal nerves. |
PHYSICAL EXAMINATION
Thorough evaluation of the larynx is paramount in preoperative selection and relies upon careful clinical examination, endoscopic evaluation, and imaging, usually computed tomography (CT) scan. The goal is to define precisely the site of origin of the cancer, to evaluate the spread of the cancer and laryngeal mobility, and to search for potential oncologic contraindications. Separate analysis of the motion of the vocal cord and arytenoid cartilages must be performed. All components of the “cricoarytenoid” unit (Fig. 26.1) should be uninvolved and have normal function. Direct laryngoscopy with magnification under apnea and no endotracheal tube present allows for the best evaluation of the status of the commissures (anterior and posterior), ventricles, and laryngeal surfaces of the epiglottis. Fine-cut CT scan of the larynx allows for precise determination of the status of the preepiglottic space, infraglottis, and cartilages. Patients with cancer arising from the true vocal cords (glottis) are candidates for a CHEP, while those with cancer considered as transglottic or supraglottic in origin as well as cancers from the anterior commissure are best managed with a CHP.
Finally, the neck is evaluated for adenopathy. Early involvement may be detected in this manner. Ipsilateral concurrent neck dissection should be considered for T3 carcinoma. Palpation of the cricothyroid and thyrohyoid membranes as well as thyroid and cricoid cartilages searches for firmness or tenderness indicating invasion by cancer.
INDICATIONS
Primary Surgery
SPCL for T1b-3 cancer (glottic, transglottic, or supraglottic in origin) of the endolarynx
Salvage surgery as a result of radiation failure for endolaryngeal cancer
CONTRAINDICATIONS
General
Inability to undergo major surgery
Respiratory insufficiency (inability to climb two flight of stairs without shortness of breath)
Major swallowing impairment (neurologic disease, stroke)
Advanced age by itself is not a contraindication, but in patients above 75 years of age, swallowing, pulmonary, and mental functions must be carefully evaluated.
Tumor Extent
Cancer arising from the epilarynx. The epilarynx also called the laryngeal margin is the junction zone between the supraglottic larynx and the other regions: the oropharynx anteriorly and the hypopharynx laterally.
Cancer originating from the subglottic region
Involvement of inter arytenoid space or posterior commissure
Mucosal involvement of both arytenoid cartilages
Subglottic extension reaching the superior border of the cricoid cartilage
Invasion of the hyoid bone and/or cricoid cartilage
Major invasion of the preepiglottic space (bulging vallecula or thyrohyoid membranes)
Fixation of the arytenoid cartilage
Extralaryngeal spread of cancer
SURGICAL TECHNIQUE
Exposure
The bed is turned 180 degrees from the anesthesia machine. The neck is slightly extended. The skin incision begins one mastoid tip to the other mastoid tip in a standard “utility flap” placed about 2-cm cephalad from the sternal notch and then extending laterally. Later in the procedure, the tracheostomy will be placed through the central portion of this incision. If a single or bilateral neck dissection is planned, this incision is extended toward the mastoid tip. A broad-based subplatysmal flap is then raised to about 1 cm above the hyoid bone. The linea alba (midline raphe) is incised, and the central compartment lymphatics from the hyoid bone to the thyroid isthmus are removed. If suspicious lymph nodes are encountered, they are sent to pathology for frozen section analysis. Lymph nodes positive for cancer at this level should lead to the completion of bilateral levels II-III neck dissection. The thyroid isthmus is identified and divided. Inferior to the thyroid, the pretracheal fascial plane is gently dissected with blunt digital manipulation, and a cervicomediastinal release of the trachea is performed, ideally down to the level of the carina. It is critical that this finger dissection is performed with care, staying in the midline overlying the anterior wall of the trachea, to avoid devascularizing the lateral or posterior blood supply of the trachea.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


