(1)
St. Johns, FL, USA
(2)
Helen Keller Foundation for Research and Education, International Society of Ocular Trauma, Birmingham, AL, USA
(3)
Consultant and Vitreoretinal Surgeon, Milos Eye Hospital, Belgrade, Serbia
(4)
Consultant and Vitreoretinal Surgeon, Zagórskiego Eye Hospital, Cracow, Poland
60.1 General Considerations1
60.1.1 Indications for Surgery
This arterial bleeding is sight-threatening if it occurs intraoperatively (ECH; see Sect. 40.1). If a limited amount of blood is present in the suprachoroidal space, the first question to answer is whether surgical intervention is necessary at all. Drainage (and PPV) should be considered in the following conditions:
“Kissing” choroidals: the hemorrhage involves opposing quadrants, and they are so high that there is retina-to-retina touch (see below and Fig. 60.1).
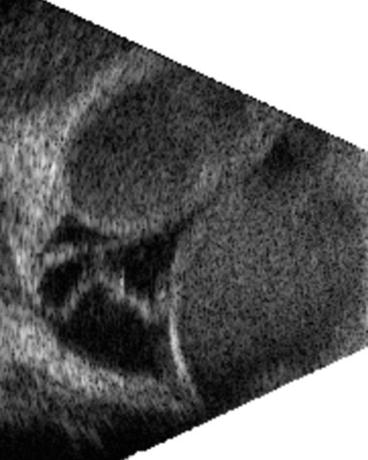
Fig. 60.1
Ultrasonography following a suprachoroidal hemorrhage. Kissing choroidals accompanied by an RD. Draining the blood is a necessary step in treating the eye, but intravitreal surgery is also needed (see the text for more details), although from this image it is impossible to determine whether what appears to be an RD is indeed a detachment (or an incomplete PVD)
Pearl
If surgery is not performed early after retina-to-retina touch developed, the adhesion between the two surfaces can quickly become so strong that they are inseparable.
High and medically uncontrollable IOP, with or without severe pain.2
Breakthrough hemorrhage: with blood in the vitreous, it is impossible to visualize the retina.
Suprachoroidal blood involving the submacular area.
Anterior displacement of the retina, with possible lens touch.
Retinal detachment.
60.1.2 Timing of Surgery
There is a window within which it is inadvisable to operate: once the blood is clotted, it is difficult or impossible to remove it. The intervention thus has to be either immediate3 or delayed until the blood liquefies, which typically takes ~10 days. Ultrasonography is helpful in determining whether liquefaction has indeed occurred.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


