Purpose
To evaluate the surgical outcomes of trabeculotomy for steroid-induced glaucoma.
Design
Multicenter, retrospective cohort study.
Methods
At 17 Japanese clinical centers, 121 steroid-induced glaucoma patients who underwent trabeculotomy between 1997 and 2006 were reviewed. Surgical failure was defined by the need for additional glaucoma surgery, deterioration of visual acuity to no light perception, or intraocular pressure ≥21 mm Hg (criterion A) and ≥18 mm Hg (criterion B). Surgical outcomes were compared with those of 108 primary open-angle glaucoma (POAG) patients who underwent trabeculotomy and 42 steroid-induced glaucoma patients who underwent trabeculectomy. Prognostic factors for failure were evaluated using the Cox proportional hazards model.
Results
The probabilities of success at 3 years for trabeculotomy for steroid-induced glaucoma vs trabeculotomy for POAG was 78.1% vs 55.8% for criterion A ( P = .0008) and 56.4% vs 30.6% for criterion B ( P < .0001), respectively. At 3 years, the success of trabeculotomy for steroid-induced glaucoma was comparable to trabeculectomy for steroid-induced glaucoma for criterion A (83.8%; P = .3636), but lower for criterion B (71.6%; P = .0352). Prognostic factors for failure of trabeculotomy for steroid-induced glaucoma were previous vitrectomy (relative risk [RR] = 5.340; P = .0452 on criterion A, RR = 3.898; P = .0360 for criterion B) and corticosteroid administration other than ocular instillation (RR = 2.752; P = .0352 for criterion B).
Conclusions
Trabeculotomy is effective for controlling intraocular pressure <21 mm Hg in steroid-induced glaucoma eyes.
Steroid-induced glaucoma is a form of open-angle glaucoma associated with various modalities of corticosteroid administration such as oral, intravenous, inhaled, ocular instilled, intravitreal, and periocular. Some histologic studies have reported the accumulation of extracellular matrices including basement membrane–like material, fine fibrillar-like material, or proteoglycans in the trabecular meshwork of steroid-induced glaucoma patients. These observations suggest that such accumulation could lead to an increased resistance to aqueous outflow in the trabecular meshwork of steroid-induced glaucoma patients.
Surgical procedures for intraocular pressure (IOP) reduction in eyes with steroid-induced glaucoma include trabeculectomy, trabeculotomy, viscocanalostomy, and laser trabeculoplasty. Although several case series have shown that these surgeries are effective for IOP reduction, surgical outcomes for steroid-induced glaucoma are not fully understood due to lack of large case-control studies aiming to investigate the success rates of trabeculotomy in steroid-induced glaucoma eyes. It has previously been reported that trabeculotomy more effectively reduces IOP in adult Japanese patients with exfoliative glaucoma than primary open-angle glaucoma (POAG). This IOP-lowering effect in eyes with exfoliative glaucoma is thought to be attributable to the relief of abnormally increased outflow resistance that was induced by the accumulation of exfoliative material within the trabecular meshwork.
For the same reason, trabeculotomy has been the surgical procedure of choice for adult patients with steroid-induced glaucoma among Japanese surgeons. We previously showed that trabeculotomy helped to reduce IOPs to 21 mm Hg or less in 14 Japanese patients with steroid-induced glaucoma. However, large-scale, comparative clinical data remain elusive on, for example, whether trabeculotomy is more effective for steroid-induced glaucoma than POAG, whether trabeculotomy for steroid-induced glaucoma offers better IOP management than other surgeries such as trabeculectomy with mitomycin C (MMC), or which characteristics of patients with steroid-induced glaucoma exhibit better prognosis after trabeculotomy. To evaluate the surgical outcomes of trabeculotomy for steroid-induced glaucoma, we retrospectively reviewed clinical charts at 17 clinical centers in Japan.
Methods
Patient Selection and Surgical Procedures
We retrospectively reviewed the medical records of patients with steroid-induced glaucoma who underwent trabeculotomy or trabeculectomy with MMC and those with POAG who underwent trabeculotomy between January 1, 1997, and December 31, 2006, at the following 17 clinical centers in Japan: Kumamoto University Hospital (Kumamoto), Niigata University Medical and Dental Hospital (Niigata), University of Tokyo Hospital (Tokyo), Kanazawa University Hospital (Kanazawa), Gifu University Hospital (Gifu), Kagawa University Hospital (Miki), University of Yamanashi Hospital (Chuo), Tohoku University Hospital (Sendai), Ryukyu University Hospital (Nishihara), Kyoto Prefectural University Hospital (Kyoto), Kagoshima University Medical and Dental Hospital (Kagoshima), Kyoto University Hospital (Kyoto), Nagoya City University Hospital (Nagoya), Saga University Hospital (Saga), Kobe University Hospital (Kobe), Hiroshima University Hospital (Hiroshima), and NTT West Kyushu Hospital (Kumamoto).
Eyes that presented with an IOP ≥22 mm Hg while on ocular hypotensive medications before surgery were included in this study. Steroid-induced glaucoma eyes were defined as open-angle eyes with an IOP elevation ≥22 mm Hg after the administration of corticosteroid. If both eyes underwent glaucoma surgeries, the eye that was treated first was investigated. Exclusion criteria were as follows: eyes with a history of previous glaucoma surgery, eyes that had undergone intraocular surgery up to 3 months before trabeculotomy or trabeculectomy, steroid-induced glaucoma eyes in the active phase of uveitis, eyes associated with IOP ≥22 mm Hg before corticosteroid administration in the medical records, and eyes that underwent combined glaucoma and cataract surgeries.
The technique of trabeculotomy performed in this study has been described previously. In brief, after conjunctival incision, a 4 × 4-mm square or triangular scleral flap at four-fifths thickness was created at the corneal limbus. After identification of the Schlemm’s canal, its outer wall was cut with a razor blade and excised with fine scissors. U-shaped probes were then inserted into both ends of the opened canal and rotated 90 degrees against the trabecular meshwork. Rotation of these probes achieved 120-degree opening of the trabecular meshwork. The scleral flap was closed with 1 to 7 10-0 nylon sutures until the wound became watertight.
During trabeculotomy, some cases were combined with a sinusotomy, based upon the procedure of Mizoguchi and associates, which made 1 or 2 sites of 1-mm-diameter sclerotomy with a punch through the scleral flap before closure with 10-0 nylon sutures. Trabeculectomy was performed according to a modification of the technique developed by Cairns. Conjunctiva incisions included limbal-based and fornix-based procedures. After the creation of a scleral flap, sponges soaked with MMC (0.4 mg/mL) were applied to the posterior surface of the conjunctiva, Tenon’s capsule, the adjacent episcleral tissue, and the scleral flap for 2 to 5 minutes, followed by irrigation with balanced salt solution. A trabecular block was excised to create a fistula in the anterior chamber, and peripheral iridectomy was then performed. The scleral flap was closed with 10-0 nylon sutures while the conjunctival flap was sutured with 10-0 nylon or 7-0 silk. All patients were required to sign informed consent forms before surgery.
Main Outcome Measure
The main outcome measure was the probability of success in the Kaplan-Meier survival-curve analysis. Before data analysis, surgical failure was defined by the following IOP levels, with or without ocular hypotensive medications, which were verified at the next visit: criterion A, IOP ≥21 mm Hg; criterion B, IOP ≥18 mm Hg. IOP data that were examined using a Goldmann applanation tonometer were collected from patients’ medical records. IOPs that corresponded to criteria A and B up to 3 months after surgery were not considered a surgical failure because of the occurrence of postoperative IOP fluctuations after trabeculotomy. If additional glaucoma surgery was performed, or visual acuity deteriorated to an absence of light perception, the eye was regarded as a surgical failure for both criteria.
We compared the surgical outcomes between the steroid-induced glaucoma with trabeculotomy group and the POAG with trabeculotomy group, and between the steroid-induced glaucoma with trabeculotomy group and the steroid-induced glaucoma with trabeculectomy group. To determine potential risk factors for surgical failure of steroid-induced glaucoma after trabeculotomy, the following variables were assessed: gender, age, pseudophakia, previous vitrectomy, route of corticosteroid administration (ocular instillation, intravitreal injection, posterior sub-Tenon’s injection, or systemic administration), duration of corticosteroid administration after glaucoma surgery, reason for corticosteroid use (collagen disease, atopic dermatitis, or uveitis), sinusotomy, previous cataract surgery, and baseline IOP. These factors were analyzed statistically in the steroid-induced glaucoma with trabeculotomy group with criteria A and B. Data on postoperative complications were also collected from the medical records.
Statistical Analysis
Data analysis was performed using the JMP version 8 statistical package program (SAS Institute, Cary, North Carolina, USA). Comparisons of the outcomes between the steroid-induced glaucoma with trabeculotomy group and the POAG with trabeculotomy group, as well as between the steroid-induced glaucoma with trabeculotomy group and the steroid-induced glaucoma with trabeculectomy group, were analyzed by the Kaplan-Meier survival curve and the log-rank test. To assess prognostic factors of steroid-induced glaucoma with trabeculotomy in univariate analysis, Kaplan-Meier survival-curve analysis and the log-rank test were used. To confirm the effects of prognostic factors and to identify the relative risk (RR) of surgical failure, multivariate prognostic factor analysis was performed with the Cox proportional hazards model. Multivariate factors were selected from variants with a probability ( P ) value of less than .15 shown by univariate analysis. A P value less than .05 was considered statistically significant.
Results
Patient Characteristics
In total, 163 patients (163 eyes) with steroid-induced glaucoma and 108 patients (108 eyes) with POAG satisfied the study criteria. All eligible patients were Japanese. Of the 163 eyes with steroid-induced glaucoma, 121 were included in the steroid-induced glaucoma with trabeculotomy group and 42 were included in the steroid-induced glaucoma with trabeculectomy group. Table 1 lists the characteristics of the enrolled patients.
| SIG-LOT, n (%) | SIG-LET, n (%) | P Value | POAG-LOT, n (%) | P Value | |
|---|---|---|---|---|---|
| (n = 121) | (n = 42) | (n = 108) | |||
| Female | 62 (51.2) | 26 (61.9) | .232 a | 38 (35.2) | .014 a |
| Right eye | 62 (51.2) | 22 (52.4) | .899 a | 50 (46.3) | .455 a |
| Age (years), mean ± SD | 38.4 ± 17.6 | 42.3 ± 17.9 | .153 b | 45.2 ± 15.0 | .001 b |
| Preoperative IOP (mm Hg), mean ± SD | 38.1 ± 10.0 | 35.6 ± 8.3 | .169 b | 28.9 ± 8.4 | <.001 b |
| Combined sinusotomy | 20 (16.5) | — | — | 33 (30.6) | .012 a |
| Previous cataract surgery | 17 (14.0) | 4 (9.5) | .626 c | 5 (4.6) | .029 c |
| Previous vitrectomy | 6 (5.0) | 0 (0.0) | .320 c | 0 (0.0) | .054 c |
| Diabetic mellitus | 13 (10.7) | 6 (14.3) | .736 c | 10 (9.3) | .709 a |
| Hypertension | 18 (14.9) | 8 (19.0) | .695 c | 15 (13.9) | .832 a |
| Cause of corticosteroid use | |||||
| Atopic dermatitis | 21 (17.4) | 4 (9.5) | .335 c | ||
| Uveitis | 25 (20.7) | 11 (26.2) | .457 a | ||
| Collagen disease | 37 (30.6) | 17 (40.5) | .240 a | ||
| Route of administration | |||||
| Ocular instillation only | 17 (14.0) | 12 (28.6) | .591 a | ||
| Posterior sub-Tenon’s injection of TA | 13 (10.7) | 1 (2.4) | .178 c | ||
| Intravitreal injection of TA | 10 (8.3) | 0 (0.0) | .121 c | ||
| Oral administration | 72 (59.5) | 26 (61.9) | .784 a | ||
| Intravenous administration | 3 (2.5) | 2 (4.8) | .826 c | ||
| Corticosteroid administration for more than 3 months after surgery | 68 (56.2) | 25 (59.5) | .708 a |
a P values are based on the χ 2 for independence test.
b P values are based on Mann-Whitney U test.
c P values are based on the χ 2 for independence test with Yates’ correction.
The steroid-induced glaucoma with trabeculotomy group was significantly younger ( P = .001) and had a higher preoperative IOP ( P < .001), a higher number of female patients ( P = .014), a higher number of previous cataract surgeries ( P = .029), and a lower number of combined sinusotomies ( P = .012) than the POAG with trabeculotomy group. However, there were no significant differences in patient characteristics between the steroid-induced glaucoma with trabeculotomy group and the steroid-induced glaucoma with trabeculectomy group.
Steroid-Induced Glaucoma vs POAG
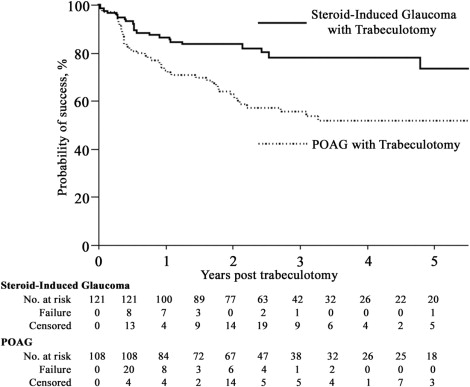
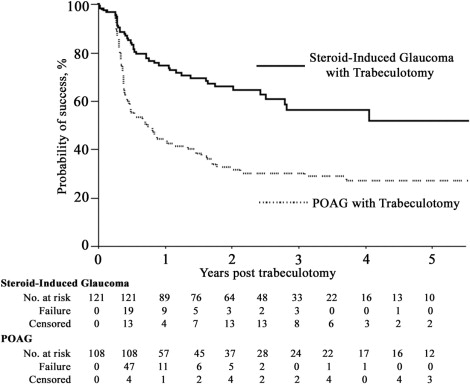
The mean follow-up periods were 38.4 ± 28.7 months in the steroid-induced glaucoma with trabeculotomy group and 49.8 ± 37.2 months in the POAG with trabeculotomy group ( P = 0.010). Kaplan-Meier survival-curve analyses of the steroid-induced glaucoma with trabeculotomy group and the POAG with trabeculotomy group for criteria A and B are presented in Figures 1 and 2 , respectively. The steroid-induced glaucoma with trabeculotomy group had a significantly higher cumulative probability of success for criteria A ( P = .0008) and B ( P < .0001). For criterion A, the probabilities of success 1, 2, 3, and 5 years after trabeculotomy in the steroid-induced glaucoma with trabeculotomy group and the POAG with trabeculotomy group were as follows: 86.5% vs 73.2%, 83.5% vs 63.0%, 78.1% vs 55.8%, and 73.5% vs 52.2%, respectively. For criterion B, the probabilities of success 1, 2, 3, and 5 years after trabeculotomy in the steroid-induced glaucoma with trabeculotomy group and the POAG with trabeculotomy group were as follows: 74.6% vs 44.7%, 66.1% vs 33.0%, 56.4% vs 30.6%, and 51.7% vs 27.5%, respectively. The number of eyes classified as surgical failures in the steroid-induced glaucoma with trabeculotomy group and the POAG with trabeculotomy group were 22/121 (18.2%) vs 45/108 (41.7%) for criterion A and 42/121 (34.7%) vs 73/108 (67.6%) for criterion B, respectively.
Since there were significant differences between the preoperative data of the steroid-induced glaucoma with trabeculotomy group and the POAG with trabeculotomy group, a Cox proportional hazards model including age, preoperative IOP, gender, previous cataract surgery, and combined sinusotomy was performed ( Table 2 ). The multivariate model suggested that trabeculotomy in steroid-induced glaucoma eyes was independently associated with a better prognosis when compared with the same procedure in POAG eyes, even after adjusting for confounding factors (criterion A, RR = 0.409, P = .0027; criterion B, RR = 0.451, P = .0005).
| Variable | Criterion A | Criterion B | ||||
|---|---|---|---|---|---|---|
| RR | 95% CI | P Value | RR | 95% CI | P Value | |
| Steroid-induced glaucoma | 0.409 | 0.223–0.735 | .0027 | 0.451 | 0.286–0.706 | .0005 |
| Age (per year) | 0.999 | 0.982–1.015 | .8917 | 1.007 | 0.995–1.019 | .2408 |
| Preoperative IOP (per mm Hg) | 1.004 | 0.977–1.029 | .7557 | 0.993 | 0.972–1.013 | .5115 |
| Female | 0.761 | 0.451–1.260 | .2911 | 0.695 | 0.468–1.021 | .0639 |
| Previous cataract surgery | 2.105 | 0.823–4.681 | .1132 | 1.627 | 0.784–3.084 | .1804 |
| Combined sinusotomy | 1.054 | 0.575–1.847 | .8600 | 0.839 | 0.526–1.300 | .4399 |
Trabeculotomy vs Trabeculectomy
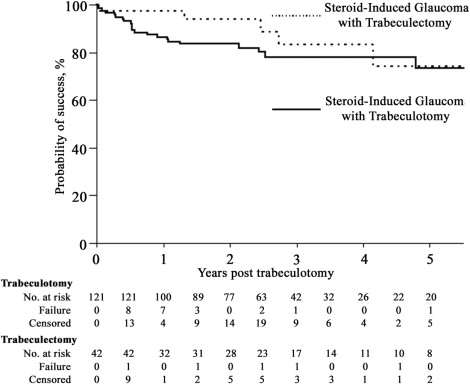
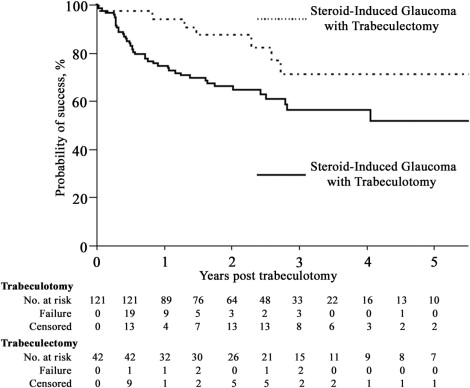
The mean follow-up period in the steroid-induced glaucoma with trabeculectomy group was 37.1 ± 31.8 months (38.4 ± 28.7 months in the steroid-induced glaucoma with trabeculotomy group, P = .808). The Kaplan-Meier survival-curve analysis between the steroid-induced glaucoma with trabeculotomy group and the steroid-induced glaucoma with trabeculectomy group for criteria A and B are presented in Figures 3 and 4 , respectively. No significant difference was found between the 2 groups for criterion A ( P = .3636). The probabilities of success 1, 2, 3, and 5 years after surgery in the steroid-induced glaucoma with trabeculectomy group for criterion A were 97.6%, 94.3%, 83.8%, and 74.5%, respectively. The number of eyes classified as surgical failures in the steroid-induced glaucoma with trabeculectomy group was 5 (11.9%) for criterion A. However, the steroid-induced glaucoma with trabeculectomy group showed a significantly higher cumulative probability of success for criterion B ( P = .0352). The probabilities of success 1, 2, 3, and 5 years after surgery in the steroid-induced glaucoma with trabeculectomy group for criterion B were 94.5%, 87.7%, 71.6%, and 71.6%, respectively. The number of eyes classified as surgical failures in the steroid-induced glaucoma with trabeculectomy group was 7 (16.7%) for criterion B.
Prognostic Factors for Failure of Trabeculotomy for Steroid-Induced Glaucoma Eyes
The potential prognostic factors influencing survival time are listed in Table 3 . Univariate analysis showed previous cataract surgery ( P = .0055) and previous vitrectomy ( P < .0001) to be significant prognostic factors for criterion A, and male gender ( P = .0422) and previous vitrectomy ( P = .0050) for criterion B. Diabetes mellitus ( P = .0848) and ocular instillation of corticosteroid ( P = .1204) were the factors with a P value of less than .15 for criterion B. The Cox proportional hazards model including these variables revealed that prognostic factors for surgical failure were previous vitrectomy (RR = 5.340, P = .0452 for criterion A; RR = 3.898, P = .0360 for criterion B) and corticosteroid administration other than ocular instillation (RR = 2.752, P = .0352 for criterion B) ( Table 4 ).
| Variable | Number of Patients | Criterion A | Criterion B | ||
|---|---|---|---|---|---|
| 80% Survival Time (Days) | P Value a | 80% Survival Time (Days) | P Value a | ||
| Gender | .1779 | .0422 | |||
| Female | 62 | >3850 | 305 | ||
| Male | 59 | 385 | 146 | ||
| Age (years) | .9040 | .2458 | |||
| <30 | 51 | 852 | 206 | ||
| ≥30 | 70 | 916 | 181 | ||
| Preoperative IOP (mm Hg) | .7443 | .4387 | |||
| <40 | 79 | 181 | 181 | ||
| ≥40 | 42 | 840 | 200 | ||
| Diabetes mellitus | .1936 | .0848 | |||
| Yes | 13 | 146 | 96 | ||
| No | 108 | 816 | 291 | ||
| Hypertension | .9394 | .9915 | |||
| Yes | 18 | >2148 | 291 | ||
| No | 103 | 852 | 195 | ||
| Combined sinusotomy | .2416 | .9270 | |||
| Yes | 20 | 146 | 120 | ||
| No | 101 | 916 | 260 | ||
| Previous cataract surgery | .0055 | .1829 | |||
| Yes | 17 | 49 | 49 | ||
| No | 104 | 1732 | 272 | ||
| Previous vitrectomy | <0.0001 | .0050 | |||
| Yes | 6 | 10 | 10 | ||
| No | 115 | 1742 | 260 | ||
| Cause of corticosteroid use | |||||
| Collagen disease | .3397 | .9248 | |||
| Yes | 37 | 750 | 195 | ||
| No | 84 | 1732 | 200 | ||
| Atopic dermatitis | .9929 | .2449 | |||
| Yes | 21 | 278 | 162 | ||
| No | 100 | 852 | 195 | ||
| Uveitis | .4674 | .7942 | |||
| Yes | 25 | >2519 | 177 | ||
| No | 96 | 840 | 200 | ||
| Route of steroid administration | |||||
| Ocular instillation only | .6968 | .1204 | |||
| Yes | 17 | 1732 | 1286 | ||
| No | 104 | 852 | 181 | ||
| Posterior sub-Tenon’s injection of TA | .9546 | .3239 | |||
| Yes | 13 | >1339 | >1339 | ||
| No | 108 | 916 | 200 | ||
| Intravitreal injection of TA | .1843 | .4379 | |||
| Yes | 10 | 49 | 49 | ||
| No | 111 | 916 | 206 | ||
| Oral administration | .7412 | .6920 | |||
| Yes | 72 | 840 | 181 | ||
| No | 49 | 1732 | 272 | ||
| Intravenous administration | .4050 | .1883 | |||
| Yes | 3 | >1580 | >1580 | ||
| No | 118 | 852 | 195 | ||
| Postoperative corticosteroid administration | .1987 | .7335 | |||
| >3 months | 68 | <3850 | 195 | ||
| ≤3 months | 53 | 372 | 200 | ||
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


