and Mitrofanis Pavlidis2
(1)
Department of Ophthalmology, Uppsala University Hospital, Uppsala, Sweden
(2)
Augencentrum Köln, Cologne, Germany
22.1 General Introduction
22.2.1 Medication
22.2.2 The Surgery Step by Step
22.2.3 Postoperative Therapy
22.2.4 Follow-Ups
22.3.1 The Surgery Step by Step
22.3.2 FAQ
22.4.3 Complications
22.4.4 FAQ
Electronic supplementary material
The online version of this chapter (doi:10.1007/978-3-319-20236-5_22) contains supplementary material, which is available to authorized users.
Electronic supplementary material
for this chapter is accessible online at http://extras.springer.com/ by searching via the ISBN.
22.1 General Introduction
Video 22.1: Submacular rtPA
Video 22.2: Traumatic submacular haemorrhage
Timing and procedure are important for this pathology. Try to treat a submacular haemorrhage within 1–2 weeks. The medication is called recombinant (tissue) plasminogen activator (rPA = rtPA, Actilyse®) and acts as a fibrinolytic agent.
There are two methods present: (1) pneumatic displacement, which comprises the intravitreal injection of rTPA, anti-VEGF and gas, and (2) vitrectomy which comprises a vitrectomy, subretinal injection of rtPA, intravitreal injection of anti-VEGF and gas.
There is an ongoing debate which method (intravitreal or subretinal rtPA) for which size of haemorrhage (small, large, massive) is superior. The actual data indicates that pneumatic displacement is superior for small haemorrhages, but it is unclear which method is the best for a large and a massive haemorrhage.
Regarding small and large haemorrhages, both methods are effective in removing the subretinal haemorrhage but only partially effective in removing the sub-RPE haemorrhage. The consequence is that an anti-VEGF therapy has to be continued after surgery. Eylea® is especially effective for a sub-RPE haemorrhage.
Note regarding a massive haemorrhage that the blood clot is attached to the underlying pigment epithelium. If you remove the blood clot with surgical extraction, you will at the same time remove the underlying pigment epithelium resulting in a geographic atrophy. The next problem is that for removal of a large blood clot, a peripheral retinectomy is required, which may result in a PVR detachment.
The definition of the size of a submacular haemorrhage varies. Our definition is as follows:
Small haemorrhage: Haemorrhage inside temporal arcades
Large haemorrhage: Haemorrhage including temporal arcades
Massive haemorrhage: Haemorrhage outside temporal arcades and haemorrhagic retinal detachment
There are several different surgical approaches available. Our procedure is as follows:
Small bleedings: Pneumatic displacement with rtPA and anti-VEGF; head down posture for 1 week. See Flow chart 22.1.
Flow chart 22.1
Our treatment algorithm for treatment of small haemorrhages
Exception: Patients who cannot perform a head down posture. Procedure: rtPA and anti-VEGF without gas.
Large bleedings: Vitrectomy with subretinal injection of rtPA and gas tamponade and anti-VEGF; head down posture for 1 week. See Flow chart 22.2.
Flow chart 22.2
Our treatment algorithm for large submacular haemorrhages
Massive haemorrhage: (1) 1–7 days preoperatively, rtPA. (2) Vitrectomy + iatrogenic hole + drainage of subretinal blood + laser + anti-VEGF + silicone oil. (3) Add rtPA in case of residual thick blood and repeat surgery 1 week later. See Flow chart 22.3.
Flow chart 22.3
Our treatment algorithm for massive submacular haemorrhages
Other surgical options:
Small and large bleedings; submacular rtPA (25micogramm in 0.2 ml) + and aspiration of blood.
Massive haemorrhage: 180–360° retinectomy + removal of haemorrhage + reattachment of retina with PFCL + laser + silicone oil; the latter surgery may cause large RPE defects because the haemorrhage is attached to the RPE.
22.2 Surgery of a Small Submacular Haemorrhage
22.2.1 Medication
1.
rtPA (Actilyse®) dose: 50 microgram/0.1 ml
2.
Anti-VEGF: 0.1 ml Avastin, Lucentis, Eylea
3.
Gas: 100 % Sf6, use alternatively air
22.2.2 The Surgery Step by Step
Inject anti-VEGF (regular dose) into the vitreous cavity. Perform a paracentesis. Inject 0.1 ml rtPA into the vitreous cavity. Then inject 0.4 ml 100 % SF6 into the vitreous cavity.
22.2.3 Postoperative Therapy
Two tablets of acetazelomide 250 mg
Head down posture for 1 week
22.2.4 Follow-Ups
Continue with Actilyse® and anti-VEGF until the haemorrhage is absorbed.
22.3 Surgery of a Large Submacular Haemorrhage
Video 22.1: Submacular Actilyse
Video 22.2: Traumatic submacular haemorrhage
22.3.1 The Surgery Step by Step
Instruments
1.
Hybrid 27G and 23G 3-port trocar system
2.
120D lens
3.
Laser probe
4.
41G subretinal injection needle (23G), DORC 1270.EXT
Usage of the 41G Subretinal Injection Needle (Figs. 22.1 and 22.2)
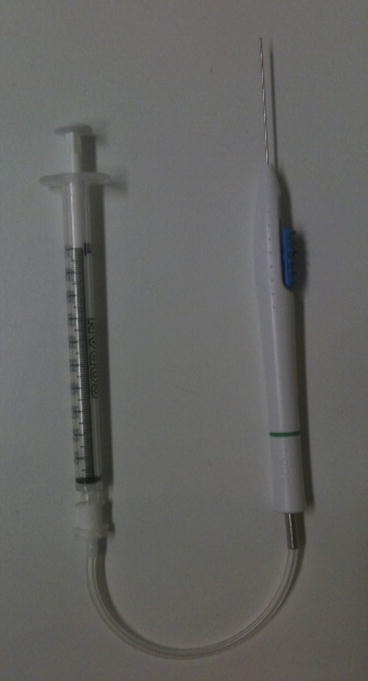
Fig. 22.1
(a) A 41G cannula. The handpiece continues with a plastic pipe. A syringe filled with rtPA is connected to this plastic pipe (DORC, 1290 BTD23). (b) The metal cannula is 23G. The 41G cannula is retractable
Fig. 22.2
The syringe with rtPA is connected to the 41G cannula
Attach the syringe with rtPA to the end of the handpiece of the 41G needle (Fig. 22.2). The surgeon holds the handpiece of the needle, and the assistant or scrub nurse holds the syringe and injects slowly the rtPA.
Remark: A 27G cannula is now available from MedOne: Poly Tip cannula 27G/38G; Indication: 38G tip for subretinal injection (MedOne, 3259)
Medication
rtPA (Actilyse®) dose: 25 microgram/0.1 ml
Anti-VEGF: 0.1 ml Avastin, Lucentis, Eylea
Tamponade:
Gas: 20 % SF6
Individual Steps
1.
Vitrectomy with PVD
2.
Subretinal injection of 0.2 ml rtPA
3.
Fluid–air exchange
4.
Tamponade with 20 % SF6
5.
Intravitreal injection of anti-VEGF
22.3.1.1 The Surgery Step by Step: Figs. 22.3, 22.4, 22.5, 22.6, 22.7 and 22.8

Fig. 22.3
A large submacular haemorrhage secondary to a CNV. Case report 11
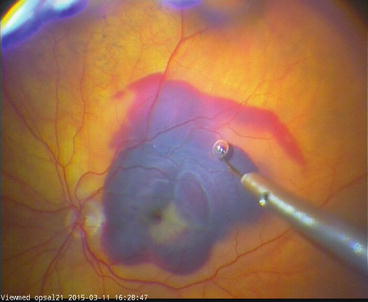
Fig. 22.4
Eject first air bubbles from the cannula, pierce the retina and inject slowly 0.2 ml rtPA. Case report 11
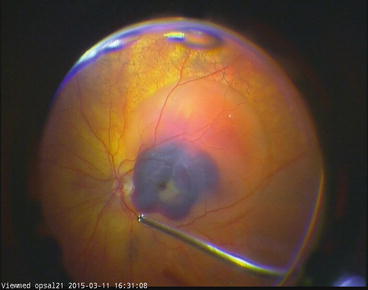
Fig. 22.5
Note the subretinal rtPA bubble. Case report 11
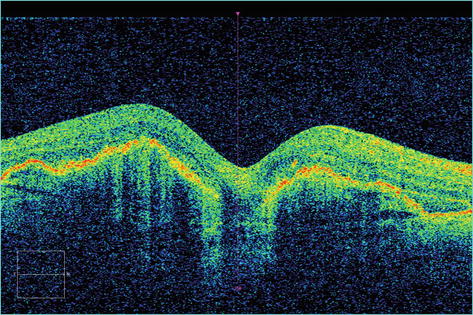
Fig. 22.6
Four-week follow-up. The subretinal haemorrhage is displaced. Case report 11
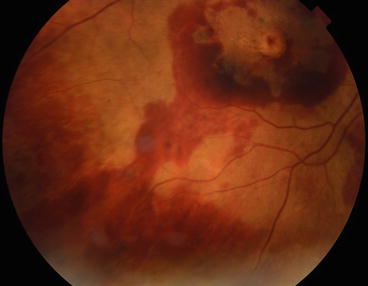
Fig. 22.7
The haemorrhage is displaced to the inferior periphery. Case report 11