Purpose
To evaluate the feasibility of split cornea transplantation for 2 recipients by combining deep anterior lamellar keratoplasty (DALK) and Descemet membrane endothelial keratoplasty (DMEK).
Design
Interventional case series.
Methods
Fifty consecutive eyes with anterior stromal disease suitable for DALK and 50 eyes with endothelial disease suitable for DMEK were scheduled for split cornea transplantation combining both procedures within 72 hours. Main outcome measures included success of using a single donor cornea for 2 recipients, best spectacle-corrected visual acuity (BSCVA), and complication rates within 6 months’ follow-up.
Results
A single donor cornea could be used for 2 recipients in 47 cases (94%). In 3 eyes (6%), the DALK procedure had to be converted to penetrating keratoplasty (PK) requiring a full-thickness corneal graft. Thereby, 47 donor corneas (47%) could be saved. Six months after surgery, mean BSCVA was 20/36 in the 47 eyes that underwent successful DALK, 20/50 in the 3 eyes that underwent conversion from DALK to PK, and 20/29 in the 50 eyes that underwent DMEK. Postoperative complications after DALK included Descemet folds in 5 eyes (11%) and epitheliopathy in 3 eyes (6%). After DMEK, partial graft detachment occurred in 26 eyes (52%) and was managed successfully with intracameral air reinjection. All corneas remained clear up to 6 months after surgery. No intraocular infections occurred.
Conclusion
Split use of donor corneal tissue for combined DALK and DMEK procedures in 2 recipients within 3 subsequent days is a feasible approach to reduce donor shortage in corneal transplantation in the future.
For over a century, penetrating keratoplasty (PK), the full-thickness replacement of a diseased cornea with an allograft donor tissue, has been the standard of care for treating advanced keratoconus, anterior stromal opacity, or endothelial failure. In the last decade, lamellar surgical techniques have been improved, allowing for selective replacement of anterior as well as posterior pathologic corneal tissue. Deep anterior lamellar keratoplasty (DALK), replacing selectively the diseased anterior part of the cornea while retaining the healthy deeper tissue, has been shown to be an effective alternative to PK in the surgical treatment of anterior stromal scars (eg, advanced keratoconus, herpetic corneal scarring) or dystrophies. For the treatment of corneal endothelial disorders (eg, Fuchs endothelial dystrophy, pseudophakic bullous keratopathy, pseudoexfoliation syndrome keratopathy), several techniques of posterior lamellar keratoplasty have been described, including deep lamellar endothelial keratoplasty, Descemet stripping automated endothelial keratoplasty (DSAEK), and Descemet membrane endothelial keratoplasty (DMEK). In DMEK, the isolated donor endothelium–Descemet membrane layer without any stroma is transplanted after stripping recipient Descemet membrane with its dysfunctional endothelium.
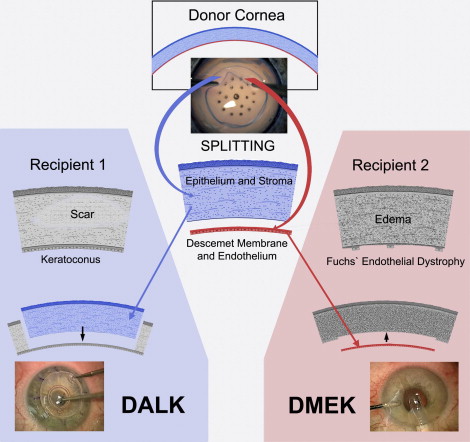
The indications for keratoplasty that can be covered by either DALK or DMEK surgery comprise approximately 80% of all indications. Since in DALK the entire donor cornea except Descemet membrane and corneal endothelium is grafted, whereas in DMEK only the donor endothelium–Descemet membrane layer is transplanted, we have recently described a split cornea transplantation approach by combining DALK and DMEK procedures in 2 recipients on the same surgery day to reduce donor shortage and cost in corneal transplantation. That means that the anterior part of the donor button (including epithelium, its basement membrane, Bowman layer, and stroma) is used for a DALK procedure, whereas the donor endothelium–Descemet membrane layer is used for a DMEK procedure in another patient. While in other areas of transplantation surgery (eg, liver transplantation) the split use of donor tissue is long established, it is a relatively novel strategy in corneal transplantation. Vajpayee and associates described in a case report the use of a single corneoscleral donor button in 3 patients. Recently, Lie and associates and our group have reported the feasibility of split cornea transplantation for 2 recipients in a small case series.
Herein, we describe the first large series using split cornea transplantation for 2 recipients. While in the beginning of our series the DMEK procedure for the patient with corneal endothelial disease was performed immediately after finishing the DALK procedure for the patient with anterior stromal disease, we now store either the posterior donor lenticule left over from a DALK procedure to complete a subsequent DMEK procedure within 72 hours or the anterior donor lenticule left over from a DMEK procedure to complete a subsequent DALK procedure within 72 hours. This would simplify the logistics of patient allocation and make split cornea transplantation more feasible in the clinical routine.
Methods
Patients
Between June 1, 2009 and May 1, 2010, 100 consecutive eyes in 100 patients (44 female and 56 male, with a mean age of 54.7 ± 17.1 years [range, 20−89 years] at the time of surgery), 50 eyes with anterior stromal disease suitable for a DALK procedure and 50 eyes with endothelial disease suitable for a DMEK procedure, were planned for split cornea transplantation at the Department of Ophthalmology, University Eye Hospital, Friedrich-Alexander University Erlangen-Nürnberg, Germany. One consecutive eye appropriate to DALK and 1 consecutive eye appropriate to DMEK were scheduled for a time interval not exceeding 72 hours.
Inclusion criteria for DALK surgery were diagnosis of advanced keratoconus (n = 47) with absence of acute hydrops, poor spectacle-corrected visual acuity (≤20/40) in the more affected eye, and contact lens intolerance or bad contact lens fit or a combination thereof, as well as diagnosis of herpetic corneal scarring (n = 3) with inactiveness for at least 2 years, absence of endothelial involvement, and poor spectacle-corrected visual acuity (≤20/40) in the more affected eye.
Inclusion criteria for DMEK surgery were diagnosis of Fuchs endothelial dystrophy (n = 48) or pseudophakic bullous keratopathy (n = 2) without significant anterior stromal scarring and poor spectacle-corrected visual acuity (≤20/40) in the more affected eye.
Eyes with any type of maculopathy (including high myopia), glaucomatous optic atrophy, or amblyopia were excluded from this prospective, nonrandomized, clinical, single-center study. Other general exclusion criteria included pregnancy and severe systemic diseases relevant to general anesthesia.
Surgical Planning
In the first half of our series, the patient with anterior stromal disease was operated on first using the DALK procedure. When bare Descemet membrane was prepared successfully without inducing large defects in DALK, the donor cornea was split into 2 parts ( Figure 1 ). The anterior part of the donor tissue (epithelium up) was used for completing the DALK surgery, and the remaining endothelium–Descemet membrane layer was stored in Dulbecco’s modified Eagle medium containing streptomycin, penicillin (Biochrom, Berlin, Germany), and fetal calf serum (Linaris, Bettingen am Main, Germany) at 34 C. This posterior lenticule of the donor cornea (endothelium down) was grafted in a second patient with corneal endothelial disease using the DMEK procedure. If a large perforation of Descemet membrane occurred accidentally during the DALK procedure that required conversion to PK using the entire donor cornea, or the split donor cornea preparation induced any defects in the endothelium–Descemet membrane layer, the second patient with endothelial failure was not canceled, but instead underwent a standard DMEK procedure using a backup donor cornea. The surgical intervention for the second patient was planned to be performed immediately after finishing the procedure for the first patient, but in case of other unplanned emergencies, the operating list was changed later within 24 hours.
Because of difficulties in the logistics of patient allocation, particularly in the availability of the patients in the clinical routine, we changed our surgical planning concept in the second half of our series. Depending on the availability of the patients, we either performed the DALK procedure first and stored the posterior donor lenticule to complete the subsequent DMEK procedure within 72 hours, or we performed the DMEK procedure first and stored the anterior donor lenticule to complete the subsequent DALK procedure within 72 hours. In this initial series of the first 100 consecutive patients a backup donor cornea was kept ready for every surgical intervention.
Altogether, the patient with anterior stromal disease was operated on first in 42 of 50 cases (84%).
Surgical and Donor Details
Under general anesthesia, deep anterior lamellar keratoplasty (DALK) based on Anwar’s big-bubble and Parthasarathy’s small-bubble technique, split donor cornea preparation, and Descemet membrane endothelial keratoplasty (DMEK) were performed by 2 surgeons (F.K. and C.C.) as described previously. If a large defect of Descemet membrane occurred accidentally during DALK procedure, a switch to PK became necessary. For the treatment of clinically significant coexisting cataract and Fuchs endothelial dystrophy (n = 20), the DMEK procedure was combined with phacoemulsification and posterior chamber lens implantation as a triple procedure. Intraocular lens power was routinely calculated by the Haigis formula using the IOLMaster (Carl Zeiss Meditec, Jena, Germany), accounting for an expected 0.5-diopter (D) hyperopic effect from the DMEK in the last 7 cases.
Phacoemulsification and implantation of an acrylic intraocular lens (in 12 cases AcriSmart 46S; Acri.Tec, Hennigsdorf, Germany, and in 8 cases AcriSof MA 60 AC; Alcon, Freiburg, Germany) into the capsular bag was routinely performed prior to the DMEK procedure.
Forty percent of the corneoscleral donor buttons were short-term cultured in Optisol-GS (Bausch & Lomb, Irvine, California, USA) at 4 C, and 60% were organ-cultured in Dulbecco’s modified Eagle medium containing streptomycin, penicillin (Biochrom, Berlin, Germany), and fetal calf serum (Linaris, Bettingen am Main, Germany) at 34 C. Donor age was 63 ± 13 years (range, 33−88 years), postmortem time was 12 ± 7 hours (range, 2−29 hours), preservation time was 331 ± 117 hours (range, 96−585 hours), and donor endothelial cell density, measured by the provider eye banks using specular microscopy, was 2574 ± 254 cells/mm 2 (range, 2050−2948 cells/mm 2 ).
After each surgery, all patients were treated topically with ofloxacin eye drops (Floxal EDO; Mann, Berlin, Germany) 4 times daily, lubricants (Hylo-Care; Ursapharm, Saarbrücken, Germany) every 2 hours, hyperosmotic eye drops (NaCl 5% Dispersa; Omnivision, Neuhausen, Switzerland) every 2 hours, and if corneal epithelium was closed, steroid eye drops (Inflanefran forte; Pharm Allergan, Ettlingen, Germany) every 2 hours. Only the mydriatic/miotic therapy differed, with pilocarpine 2% eye drops (Bausch & Lomb) being given 5 times daily after DMEK and DALK for as long as air was in the anterior chamber and cycloplegic eye drops (cyclopentolate 1%; Alcon) being given twice a day after PK for 1 week. Systemic corticosteroid therapy (Solu-Decortin H 150 mg; Merck Pharma, Darmstadt, Germany) was tapered over 1 week. The topical antibiotic was discontinued 1 week after surgery, and the other eye drops were tapered gradually based on the clinical outcome. In case of herpetic corneal scarring, the postoperative treatment regimen was complemented by topical acyclovir ointment 3% (Zovirax; GlaxoSmithKline, Munich, Germany) being given 5 times daily and tapered gradually with the other eye drops based on the clinical outcome, as well as by oral acyclovir 400 mg (Acic; Hexal, Holzkirchen, Germany) 5 times daily for 6 weeks and thereafter twice a day for a total of 12 months.
Clinical Assessment and Main Outcome Measures
Standardized eye examinations, including measurement of Snellen uncorrected visual acuity and best spectacle-corrected visual acuity (BSCVA), slit-lamp examination, tonometry, funduscopy, subjective refractometry (trial glasses in a trial frame), standard keratometry (Ophthalmometer, type H, 190071; Carl Zeiss Meditec), corneal topography (TMS-1; Tomey, Erlangen, Germany), corneal pachymetry (Pentacam; Oculus, Wetzlar, Germany), specular microscopy of endothelial cell density (SeaEagle; Hightec American Industrial Laboratories, Lexington, Massachusetts, USA), and slit lamp–adapted optical coherence tomography of the anterior segment (Heidelberg Engineering, Lübeck, Germany) were carried out by 1 of 4 investigators (L.H., S.R., B.B., or K.L.) before surgery as well as 1 day, 1 week, 4 weeks, and 3, 6, and 12 months after surgery. All patients reached a minimum follow-up of 6 months. Intraoperative and postoperative complications, as well as secondary interventions (such as intracameral air injection), were recorded. Before and after each surgery all culture media with the corneoscleral donor tissue were examined microbiologically to exclude any contamination.
Main outcome measures included success of using a single donor cornea for 2 recipient eyes, visual and refractive outcomes, endothelial cell density, and pachymetry, as well as intraoperative and postoperative complication rates.
Commercial software (SPSS version 15.0 for Windows; SPSS, Inc, Chicago, Illinois, USA) was used for all statistical analyses. BSCVA results were analyzed in logarithm of the minimal angle of resolution (logMAR) equivalent units.
Results
Saving of Donor Cornea Tissue
Using split cornea transplantation by combining a DALK and a DMEK surgery within 72 hours, a single donor cornea could be used for 2 recipients in 47 of 50 cases (94%). Split donor cornea preparation was performed successfully in all 50 cases (100%) without inducing significant central defect in the endothelium–Descemet membrane layer. After split donor cornea preparation, the anterior donor lenticule was used for the DALK procedure immediately in 39 eyes, and the posterior donor lamella was stored for a mean time interval of 13.5 ± 16.7 hours (range, 2−68 hours) to complete the subsequent DMEK procedure. In 8 cases the posterior donor lamella was inserted immediately during the DMEK procedure, and the anterior donor lenticule was stored for a mean time interval of 10.4 ± 8.3 hours (range, 2−24 hours) to complete the subsequent DALK procedure. In 3 of the 50 eyes with anterior stromal disease (6%), the DALK procedure had to be converted to PK requiring a full-thickness corneal graft because of accidental macroperforation of recipient Descemet membrane. All 50 patients with corneal endothelial failure underwent DMEK surgery, requiring a backup donor cornea in 3 patients (6%) because of conversion of the previous DALK procedure to PK. Thereby, 100 patients with advanced corneal diseases could be transplanted using 53 donor corneas, so that a total of 47 donor buttons (47%) could be saved.
Visual and Refractive Outcomes
In the 47 eyes that underwent the DALK procedure successfully, the mean BSCVA was 0.79 ± 0.18 logMAR (range, 0.5−1.0 logMAR) before surgery and improved to 0.45 ± 0.11 logMAR (range, 0.2−0.7 logMAR) at 1 month, to 0.30 ± 0.10 logMAR (range, 0.1−0.5 logMAR) at 3 months, and to 0.25 ± 0.10 logMAR (range, 0.1−0.4 logMAR) at 6 months after surgery ( Figure 2 , Left). The mean 6-month BSCVA was 0.25 ± 0.11 logMAR (range, 0.1−0.4 logMAR) in the case of using a non-stored anterior donor lenticule, and 0.25 ± 0.09 logMAR (range, 0.1−0.4 logMAR) in the case of using a stored anterior donor lenticule. The mean spherical equivalent decreased from −3.9 ± 2.7 D (range, −10.5 to 0.0 D) before surgery to −1.4 ± 1.2 D (range, −4.5 to 0.0 D) at 6 months after surgery, and the refractive astigmatism decreased from 2.8 ± 2.3 D (range, 0.0 to 8.5 D) before surgery to 1.2 ± 0.9 D (range, 0.5 to 3.5 D) at 6 months after surgery.
In the 3 eyes that underwent conversion to PK during DALK surgery, the mean BSCVA averaged 0.93 ± 0.12 logMAR (range, 0.8−1.0 logMAR) before surgery, 0.57 ± 0.06 logMAR (range, 0.5−0.6 logMAR) at 1 month, 0.47 ± 0.06 logMAR (range, 0.4−0.5 logMAR) at 3 months, and 0.40 ± 0.10 logMAR (range, 0.3−0.5 logMAR) at 6 months after surgery. The spherical equivalent was −3.2 ± 1.0 D (range, −4.0 to −2.0 D) before surgery and −0.7 ± 0.8 D (range, −1.5 to 0.0 D) at 6 months after surgery, and the refractive astigmatism was 2.7 ± 0.8 D (range, 2.0−3.5 D) before surgery and 0.5 ± 0.5 D (range, 0.0−1.0 D) at 6 months after surgery.
In the 50 eyes that underwent the DMEK procedure successfully, the mean BSCVA was 0.72 ± 0.20 logMAR (range, 0.3−1.0 logMAR) before surgery and improved to 0.37 ± 0.11 logMAR (range, 0.2−0.6 logMAR) at 1 month, to 0.26 ± 0.13 logMAR (range, 0.0−0.5 logMAR) at 3 months, and to 0.16 ± 0.16 logMAR (range, −0.1 to 0.4 logMAR) at 6 months after surgery ( Figure 2 , Right). Up to 6 months after DMEK surgery, 15 eyes (30%) recovered 20/20 or better vision, 19 eyes (38%) had 20/25 or better vision, and 42 eyes (84%) had 20/40 or better vision. The mean 6-month BSCVA was 0.08 ± 0.10 logMAR (range, −0.1 to 0.2 logMAR) in the case of using a non-stored posterior donor lenticule, and 0.18 ± 0.16 logMAR (range, −0.1 to 0.4 logMAR) in the case of using a stored posterior donor lenticule. In the 30 eyes that underwent a stand-alone DMEK procedure, the mean 6-month BSCVA averaged 0.17 ± 0.16 logMAR (range, −0.1 to 0.5 logMAR), and in the 20 eyes that underwent a triple DMEK procedure 0.18 ± 0.19 logMAR (range, −0.1 to 0.5 logMAR). The mean spherical equivalent averaged 0.1 ± 2.0 D (range, −3.5 to 4.0 D) before surgery and 0.9 ± 1.3 D (range, −2.8 to 3.0 D) at 6 months after surgery. In the 30 eyes that underwent a stand-alone DMEK procedure, the mean change in spherical equivalent from before surgery to 6 months after surgery was +0.9 ± 1.3 D (range, −2.5 to 4.3 D), and in the 20 eyes that underwent a triple DMEK procedure +0.7 ± 2.6 D (range, −3.8 to 4.5 D). The refractive astigmatism was 0.5 ± 0.6 D (range, 0.0−2.0 D) before surgery and 0.6 ± 0.6 D (range, 0.0−2.5 D) at 6 months after surgery.
Endothelial Cell Density and Pachymetry
In the 47 eyes that underwent the DALK procedure successfully, the mean endothelial cell density was 2125 ± 165 cells/mm 2 (range, 1852−2378 cells/mm 2 ) before surgery and decreased to 2059 ± 134 cells/mm 2 (range, 1803−2200 cells/mm 2 ) at 1 month, to 2014 ± 137 cells/mm 2 (range, 1795−2165 cells/mm 2 ) at 3 months, and to 1979 ± 130 cells/mm 2 (range, 1777−2122 cells/mm 2 ) at 6 months after surgery ( Figure 3 , Left).
The postoperative endothelial cell loss was 6.7% ± 4.1% (range, 1.2%−15.8%) up to 6 months after DALK. The preoperative central corneal thickness averaged 412 ± 57 μm (range, 318−498 μm), and the postoperative central corneal thickness averaged 515 ± 32 μm (range, 480−572 μm) within 6 months’ follow-up.
In the 3 eyes that underwent conversion to PK during DALK surgery, the mean endothelial cell density was 2236 ± 157 cells/mm 2 (range, 2085−2399 cells/mm 2 ) before surgery, 2250 ± 335 cells/mm 2 (range, 2002−2632 cells/mm 2 ) at 1 month, 2192 ± 299 cells/mm 2 (range, 1952−2527 cells/mm 2 ) at 3 months, and 2140 ± 296 cells/mm 2 (range, 1930−2478 cells/mm 2 ) at 6 months after surgery. In comparison with the donor endothelial cell density, the mean cell loss was 18.8% ± 8.8% (range, 11.5%−28.6%) up to 6 months after keratoplasty. The central corneal thickness was preoperatively 395 ± 54 μm (range, 339−446 μm), and at 6 months postoperatively 576 ± 11 μm (range, 565−587 μm).
In the 50 eyes that underwent the DMEK procedure successfully, the mean endothelial cell density was 1657 ± 233 cells/mm 2 (range, 1114−2051 cells/mm 2 ) at 1 month, 1576 ± 251 cells/mm 2 (range, 1072−1989 cells/mm 2 ) at 3 months, and 1506 ± 243 cells/mm 2 (range, 1047−1931 cells/mm 2 ) at 6 months after surgery ( Figure 3 , Right). In comparison with the donor endothelial cell density of 2570 ± 258 cells/mm 2 (range, 2050−2948 cells/mm 2 ), the mean cell loss was 34.8% ± 11.7% (range, 9.7%−58.7%) at 1 month, 37.9% ± 12.4% (range, 12.1%−61.8%) at 3 months, and 40.7% ± 12.1% (range, 15.8%−61.2%) at 6 months after DMEK. The mean 6-month endothelial cell loss was 42.1% ± 11.2% (range, 25.9%−60.7%) in the case of using a non-stored posterior donor lenticule, and 40.3% ± 12.4% (range, 15.8%−61.2%) in the case of using a stored posterior donor lenticule. In the 30 eyes that underwent a stand-alone DMEK procedure, the mean 6-month endothelial cell loss was 38.8% ± 13.3% (range, 15.8%−61.2%), and in the 20 eyes that underwent a triple DMEK procedure 43.5% ± 9.6% (range, 29.0%−60.7%). The central corneal thickness averaged 723 ± 86 μm (range, 603−893 μm) before surgery, and 534 ± 43 μm (range, 443−611 μm) during 6-month follow-up.
Intraoperative and Postoperative Complications
During DALK surgery for the 50 eyes with anterior stromal disease, accidental macroperforation of Descemet membrane requiring conversion to PK occurred in 3 eyes (6%). Intraoperative microperforation, managed with an intracameral air injection at the end of surgery, was encountered in 4 of the 50 patients (8%). Postoperative Descemet folds were diagnosed in 5 of 47 eyes (11%) eyes after successful DALK, and epitheliopathy after delayed corneal epithelial wound healing was diagnosed in 3 of 47 eyes (6%). Other well-known complications, such as primary failure, acute rejection, infectious keratitis, interface opacity, Urrets-Zavalia syndrome, or loose sutures, were not observed during follow-up ( Figure 4 , Top left and right). The postoperative complication rate was 18% (7/39) in the case of using a non-stored anterior donor lenticule and 13% (1/8) in the case of using a stored anterior donor lenticule.



