Patients seeking facial rejuvenation surgery are frequently apprehensive about their postoperative appearance. They express concern about looking too different, not themselves, or being recognized for having had “something done.” Invariably they will mention not wanting to resemble a particular public figure or express hesitation because of scars or deformities seen in a neighbor, relative, or passerby. Consequently, patients who seek facial rejuvenation surgery are essentially requesting two desired outcomes—a natural more youthful appearance within their current facial identity and the absence of noticeable scarring and irregularities, thereby avoiding the associated problems of camouflaging, altered hairstyles, and public scrutiny.
To achieve these desired outcomes while minimizing the stigmata of surgery, the techniques described herein have been applied and proven successful in the senior author’s (K.J.E) 20-year facial rejuvenation practice.
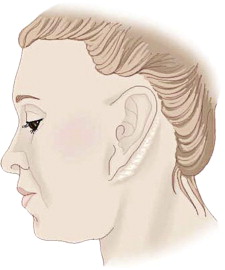
Stigmata to avoid
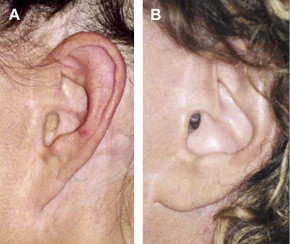
The most recognizable stigmata of facial rejuvenation surgery are unnatural hairlines, tragal distortions, ear lobule deformities, irregular neck contours, and an overall look of being lifted ( Fig. 1 ). These problems can be avoided by a careful preoperative analysis followed by adherence to specific incision designs and techniques, a meticulous attention to detail, and a governing philosophy that strives for a natural youthful appearance. The specific techniques and philosophy to prevent these stigmata are presented in this article in a problem-specific format.
Incisions
Hairline incisions
The objectives for the hairline include the prevention of temporal hair loss and the re-establishment of a natural appearing postauricular hairline. Achieving both of these goals significantly impacts patient satisfaction because success allows versatility in hairstyle selection and freedom from camouflaging.
To achieve these goals, the hairline is scrutinized preoperatively. The temporal tuft is assessed for position and density, which determines the placement of incisions. For temporal hairlines that extend to the level of the helical root or lower, a linear incision extending superiorly into the temporal area is used ( Fig. 2 ). Other surgeons have reported superior results using curvilinear designs or incisions that proceed horizontally across the temporal tuft . This departure is based on concerns about a more visible scar, unnatural hair parting along the linear incision, or loss of the temporal hair tuft (alopecia). These concerns regarding linear incisions have not been witnessed in the authors’ patients with long-term follow-up. The complications associated with linear incisions are more likely secondary to other factors, such as excessive electrocautery, the improper handling of tissues, or undue tension during closure leading to scar widening.
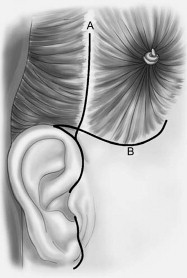
Patients with higher preoperative temporal tufts, especially those above the superior helical rim, have incisions designed to prevent further elevation of the temporal tuft ( Fig. 2 ). Elevating the tuft in these circumstances would create a noticeable distortion of the hairline easily recognized by the lay public. The incision performed is a classic tricho-phytic incision beveled superiorly. To provide a thin imperceptible scar, the closure needs to be tension free, which places a premium on flap elevation and the excision of redundant skin. This meticulous attention to detail is continued during closure, which is completed using interrupted non-absorbable sutures. The sutures are removed no later than postoperative day 5.
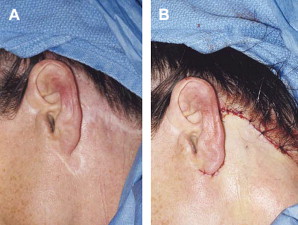
For the postauricular hairline, the incision is designed to be inconspicuous and to create a hairline that is natural and free of step-off or irregularities. Incisions that circumnavigate the hairline and those positioned within the postauricular sulcus are often noticed postoperatively. All too often, these scars migrate inferiorly, widen, or become hyper-trophic. The scars are easily recognized in public and become a source of considerable embarrassment to the patient. As a result, patients are compelled to camouflage the scars with make-up or restrictive hairstyles—no longer free to wear their hair up. The surgeon must recognize and fully appreciate this lack of versatility in hairstyling to the patient’s overall satisfaction. Additionally, scar revision in this area can be extremely difficult, often necessitating revision rhytidectomy, with only modest improvement expected in more severe cases ( Fig. 3 ).
To prevent postauricular hairline distortions, the postauricular portion of the incision should course above the postauricular sulcus, rising superiorly onto the eminence of the concha cymba. At this level, the incision turns posterior into and through the hairline ( Fig. 4 ). While in the hair, the incision does not mirror the hairline and proceed inferiorly; rather, it stays more superior and horizontal, such as on a course to meet the inferior nuchal line. This incision design provides an excellent superior vector of pull during closure and rotational mobility of the flap, allowing for easy recreation of a postauricular hairline without step-off.

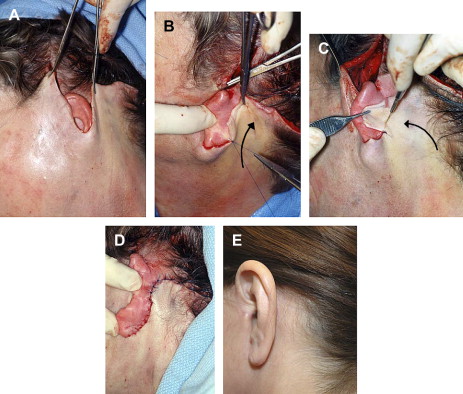
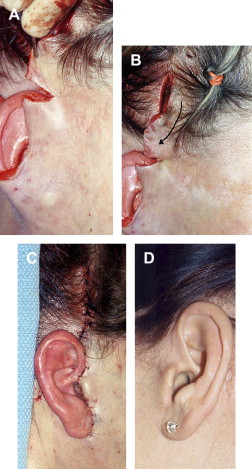
After extensive undermining and imbrication of the superficial musculoaponeurotic system (SMAS), closure is started in the postauricular area. The skin flaps are positioned on either side of the auricle ( Fig. 5 A). Closure of the postauricular hairline consists of two distinct maneuvers. First, the auricle is reflected forward by the assistant, and the postauricular flap is grasped and pulled firmly in a more superior and slightly posterior direction. The anterior leading edge of the postauricular flap is incised just below the superior most portion of the postauricular incision, which is high on the eminence of the concha cymba. The length of the incision is determined by the amount of excess skin to be excised. The apex of this incision is then sutured just below the superior most portion of the postauricular incision ( Fig. 5 B). Next, the posterior portion of the flap is rotated anteriorly, removing excess tissue as needed ( Fig. 5 C). The rotation offers the surgeon the ability to realign the hairline with minimal difficulty. The incision is closed with interrupted nonabsorbable sutures in the hair, and absorbable sutures are placed in the immediate postauricular area. No staples are used. There is often some puckering within the hair closure, but this resolves quickly during the postoperative period. Proper execution of this technique will readily produce a hairline without step-off and a well-concealed incision ( Fig. 5 D).
For closure of the temporal hairline (linear incision), the preauricular flap is pulled in a postero-superior direction. The posterior leading edge of the flap is incised at the level of the zygomatic root, with the length of the incision dependent on the amount of skin requiring removal ( Fig. 6 A). After the apex of the incision is sutured, the redundant tissue is pulled in an inferoposterior direction ( Fig. 6 B). The excess skin is resected, which typically results in opposite edges of unequal length. A meticulous closure with interrupted nonabsorbable sutures will result in a well-concealed incision and a natural appearing hairline ( Fig. 6 C).
Preauricular and tragal incisions
The goals of preauricular and peritragal incisions are inconspicuous scars and minimal distortions of the tragus. Commonly, the designs of peritragal incisions are based largely on the patient’s gender. Posttragal incisions are used in female patients but are seldom applied to male patients. Nevertheless, this dogma may be changing. The authors have witnessed an increase not only in male patients requesting facial rejuvenation surgery but also in specific requests for a posttragal incision. These requests are driven by the desire for the complete concealment of all incisions and other stigmata of facial rejuvenation surgery. As a result, the number of pretragal incisions performed on male patients has substantially decreased in the authors’ patient population.
Pretragal incisions are still used in patients with postoperative concerns about hearing aid fit and in men with heavy dark beards or those unwilling to perform daily hair removal or to undergo laser removal of hair-bearing skin that is subsequently positioned into the tragal area. However, most men are willing to perform the necessary daily maintenance to have a better concealed incision.
The literature is scarce regarding techniques detailing preauricular and peritragal incisions. To identify objectively the best incision design for the peritragal area, a histologic study of tragal anatomy and a retrospective evaluation of postoperative outcomes of tragal incisions were performed at the authors’ center . The purpose of the studies was to evaluate peritragal anatomic features that may predispose certain patients to less than optimal results with standard posttragal incisions. The well-known complications of posttragal incisions are termed tragal elimination and include the postoperative changes listed in Box 1 .
Anteriorly displaced tragus
Abnormal meatal show
Tragal blunting
Blunting of anterior incisure (webbing)
Narrowing of intertragal incisure (webbing)
Loss of preauricular sulcus
Loss of tragal height
The study by Kallman and coworkers highlighted many interesting findings that may assist the facial plastic surgeon. Preoperative analysis should recognize certain anatomic features within the peritragal area ( Fig. 7 ). For instance, patients with poorly defined anterior incisura or prominent supratragal tubercles and intertragal incisura pose an increased risk for peritragal abnormalities such as supratragal and inferior tragal webbing, respectively ( Fig. 8 ). However, a standard posttragal incision for all patients is problematic and should be customized to the patient’s particular anatomy. In patients with poorly defined anterior incisura or prominent supratragal tubercles, the incision should be angulated within the anterior incisura before proceeding inferiorly onto the posterior portion of the tragus. The angulation serves to irregularize the incision and reduce the incidence of supratragal webbing. In patients with prominent intertragal incisura, the surgeon should intentionally avoid the intertragal incisura by immediately carrying the incision from the posterior tragal area superior to the prominent intertragal incisura, assuming a more pretragal incision pattern before proceeding inferiorly ( Fig. 9 ).

The incision design is a modification of that described by Marten but is used only for patients with the peritragal differences stated previously, that is, shallow anterior incisura, prominent supratragal tubercles, and intertragal incisura. Otherwise, the incision adheres to the more traditional curvilinear design. That is, the course follows the natural contour of the insertion of the helical crus, proceeding inferiorly just posterior to the free edge of the tragus before exiting through the middle of the intertragal incisura onto the lobular crease ( Fig. 9 ). This more traditional incision maximizes the segment behind the tragus, offering superior camouflage in the preauricular region.
The posttragal portion of the incision is positioned 3 to 4 mm behind the tragus. Elevation of the tragal flap is in the subcutaneous plane just above the perichondrium. Dissection should be careful and avoid penetration of the perichondrium and any damage to the underlying cartilage.
The cause of tragal blunting has been hypothesized to be secondary to differences in dermal thickness between the cheek and tragal skin. As cheek skin is brought into the peritragal area during skin resection, the increased thickness of dermis in the cheek skin would blunt the normal architecture of the tragus despite defatting maneuvers. Nevertheless, the authors’ histologic analysis found no statistical difference between the dermal thickness of cheek and tragal skin, and the clinical evaluation found no anatomic features that predisposed patients to tragal blunting; therefore, prevention of tragal blunting is a matter of surgical technique. The authors’ technique includes defatting the skin flap, typically up to 1 cm anterior to the tragus. Additionally, the SMAS flap is trimmed and sutured to rest approximately 1 cm anterior from the base of the tragal cartilage, helping to preserve the pretragal sulcus. The use of pretragal tacking sutures is recommended as well as a tension-free closure. The preauricular incision is closed with interrupted nonabsorbable sutures; absorbable sutures are used for the posttragal portion of the incision. These techniques will help reduce the postoperative sequela of tragal elimination.
Ear lobule incision
The creation of a pixie or satyr ear deformity is preventable ( Fig. 10 ). The causes for this deformity typically include improper incision placement around the lobule, aggressive skin removal, or excessive tension at the time of closure.



