Over the last decade, lower transconjunctival blepharoplasty has become the method of choice used by facial plastic surgeons for the treatment of lower eyelid herniated fat owing to the reduced rate of complications and the hidden incision . The primary complications of the transcutaneous approach are lower lid retraction with scleral show, lower lid ectropion, and rounding of the lateral canthal angle .
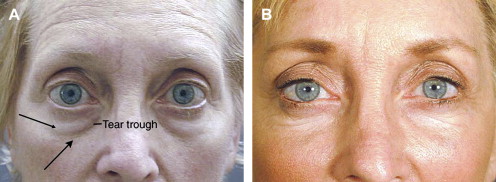
Traditionally, lower eyelid herniated fat is removed, which may cause a sunken or hollow lid appearance, especially in patients with a tear-trough deformity. A tear-trough deformity or nasojugal fold is usually caused by the inferior descent of the cheek (malar mound) with age or an anatomic bony deficiency of the maxilla, producing a depression at the medial inferior orbital rim ( Fig. 1 ) . Additionally, the midface descends, creating a double-convexity contour deformity (lower eyelid herniated orbital fat convexity followed by the cheek/malar mound convexity) ( Fig. 2 ). Fat preservation in the lower eyelid, which was originally described in 1996, may prevent some of these contour irregularities . Fat repositioning is defined as the subperiosteal repositioning of the medial and central lower lid herniated orbital fat into the nasojugal fold. The lateral orbital fat pad may be repositioned into the lateral inferior orbital region if needed.

Advantages of fat repositioning include prevention or improvement of a tear-trough deformity and treatment of the herniated orbital fat. The disadvantages of fat repositioning are the steep learning curve and potential complications such as diplopia owing to injury of the inferior oblique muscle, fat granulomas, prolonged edema, and, rarely, soft-tissue irregularities.
Candidates for fat repositioning include patients with the following:
- •
Lower eyelid herniated fat
- •
Presence of a tear-trough deformity
- •
Acceptance of the possible risks and complications
- •
Realistic expectations
Often, this technique is used to soften moderate-to-severe tear-trough deformities in patients with minimal to no herniated fat because the fat may be released once the septum is opened. In addition, a lower eyelid skin pinch may be performed in patients with excess skin in the lower lid and adequate lower lid tone. Often, lower eyelid fat repositioning is combined with a subperiosteal midface-lift to rejuvenate completely the lower eyelid-cheek region.
Surgical technique
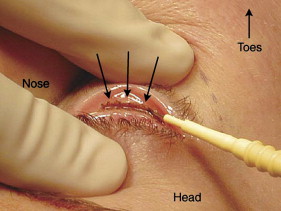
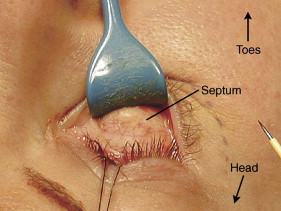
Transconjunctival fat repositioning is performed with the patient under local or general anesthesia. With the patient in the supine position, a surgical marker is used to mark the nasojugal groove. One drop of tetracaine ophthalmic solution is instilled in each eye. One percent lidocaine (Xylocaine) with 1:100,000 epinephrine is injected into the lower conjunctival surface and subcutaneously and sub-periosteally over the inferior orbital rim nasal to the nasojugal fold. With the use of a Desmarres retractor, the lower conjunctival area is exposed. The preseptal approach involves a transconjunctival incision at the inferior edge of the tarsus using a Colorado needle ( Fig. 3 ). The incision is carried through the lower eyelid retractors with care taken not to injure the tarsus. A preseptal dissection ( Fig. 4 ) is performed bluntly with surgical q-tips.
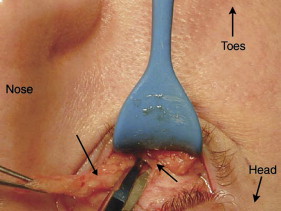
A 4-0 black silk traction suture is placed through the posterior conjunctival flap to protect the cornea and to aid with exposure of the fat pads. With slight pressure on the globe, the medial fat is identified. With the Colorado needle, a buttonhole is made in the septum exposing the medial fat pad. The fat is made into a pedicle for repositioning by thinning and elongating it with careful dissection of the surrounding fibrous attachments. The base of the pedicle is kept intact to ensure viability of the fat pad. While grasping the fat pad with forceps, blunt dissection is performed using q-tips or scissors between the fat pad and the inferior oblique muscle to ensure that the fat pad is not adherent to the inferior oblique muscle ( Fig. 5 ). This maneuver prevents tethering of the muscle to the fat pad during repositioning. During the entire dissection, meticulous dissection and hemostasis helps prevent injury to the inferior oblique muscle.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


