Purpose
To explore the relationship of sleep apnea and the subsequent development of retinal vein occlusion (RVO).
Design
A retrospective nonrandomized, matched-control cohort study using the Taiwan National Health Insurance Research Database.
Methods
From 1997 through 2007, we identified newly diagnosed sleep apnea cases in the database. A control group without sleep apnea, matched for age, gender, and comorbidities, was selected for comparison. The 2 cohorts were followed up, and the occurrence of RVO was observed.
Results
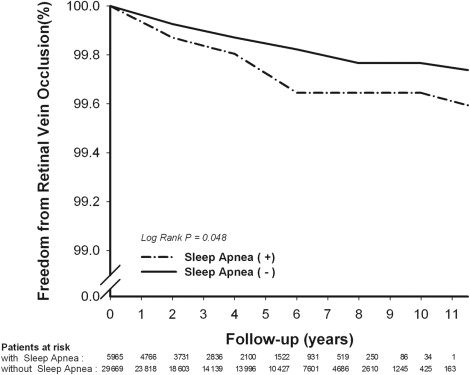
Of the 35 634 sampled patients (5965 sleep apnea patients vs 29 669 controls), 52 (0.15%) experienced RVO during a mean follow-up period of 3.72 years, including 13 (0.22%, all branch RVO) from the sleep apnea cohort and 39 (0.13%, 39 branch RVO and 10 central RVO) from the control group. Kaplan-Meier analysis revealed the tendency of sleep apnea patients toward RVO development ( P = .048, log-rank test). Patients with sleep apnea experienced a 1.94-fold increase (95% confidence interval, 1.03 to 3.65; P = .041) in incident RVO, which was independent of age, gender, and comorbidities.
Conclusions
Sleep apnea may be an independent risk factor for RVO.
Sleep apnea is a common disorder characterized by cessation of breath during sleep, which is mostly attributed to repetitive upper airway collapse (namely, obstructive sleep apnea). Obstructive sleep apnea is estimated to affect 24% of men and 9% of women of the middle-aged population in the United States and is associated with a variety of cardiovascular diseases, such as hypertension, coronary artery disease, arrhythmia, and stroke.
Retinal vein occlusion (RVO), the second most frequent retinal vascular disorder, shares some common risk factors with sleep apnea. In addition to the well-known risk factors of RVO, including hypertension, diabetes mellitus, and glaucoma, sleep apnea recently was reported by Glacet-Bernard and associates as another possible risk factor, based on their study showing a high prevalence of sleep apnea in patients with RVO.
However, the aforementioned study had the limitations of cross-sectional design without prospective follow-up, small sample size, and lack of an appropriate control group, dampening its statistical power. We hypothesized sleep apnea may contribute independently to RVO, and conducted this nationwide population study to investigate the relationship between sleep apnea and the subsequent development of RVO.
Methods
Database
The National Health Insurance program in Taiwan has operated since 1995 and has enrolled upwards of 97% of the inhabitants in Taiwan. The National Health Insurance Research Database (NHIRD) at the National Health Research Institutes ( http://www.nhri.org.tw/nhird/ ) in Miaoli, Taiwan, is in charge of the entire National Health Insurance claims database, and it has published numerous extracted data sets for researchers. The National Health Research Institutes released a cohort data set of 1 000 000 randomly sampled people with all their records from 1995 onward. It is one of the largest nationwide population-based databases in the world. These samples were confirmed by the National Health Research Institutes to be representative of the Taiwanese population. In this cohort data set, each patient’s original identification number has been encrypted to protect privacy. Despite this, the linkage of claims belonging to the same patient is feasible within the NHIRD data sets owing to the consistent encryption procedure. To our knowledge, NHIRD is one of the largest nationwide population-based databases in the world, and more than 800 scientific papers have been published using its data.
Study Sample and Control
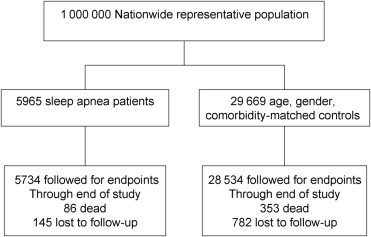
We identified patients who were newly diagnosed with sleep apnea (International Classification of Diseases, Ninth Revision, Clinical Modification [ICD-9-CM] codes 780.51, 780.53, and 780.57) from the 1 000 000 sampling cohort data set from January 1, 1997. By stratified random sampling, an age-, gender-, and comorbidity-matched control group was selected from those without sleep apnea throughout the entire course of follow-up. In both groups, patients with pre-existing RVO (ICD-9-CM codes 362.35 or 362.36) before enrollment were excluded. The variables to be matched included age, sex, and pre-existing (on enrollment) hypertension (ICD-9-CM codes 401.xx through 405.xx), diabetes mellitus (ICD-9-CM code 250.xx), coronary artery disease (ICD-9-CM codes 410.xx through 414.xx), glaucoma (ICD-9-CM codes 364.22, 365.xx, 366.31, 377.14), chronic kidney disease (ICD-9-CM codes 580.xx through 587.xx), chronic obstructive lung disease (ICD-9-CM codes 491, 492, 494, 496), asthma (ICD-9-CM code 493.xx), arrhythmia (ICD-9-CM codes 427.xx, 785.0, 785.1), ischemic stroke (ICD-9-CM codes 433.xx through 434.xx, 436, 437.1), and hyperlipidemia (ICD-9-CM code 272.xx). Both the sleep apnea cohort and control cohort were followed up from enrollment to the date of diagnosis of RVO, death, withdrawal from the insurance, or December 31, 2007 ( Figure 1 ).
Main Outcome Measures
The end point of the study was defined as occurrence of RVO (ICD-9-CM codes 362.35 or 362.36).
Statistical Analysis
A Microsoft SQL Server 2005 (Microsoft Inc, Redmond, Washington, USA) was used for data management and computing. Statistical analysis was performed using SPSS software version 15.0 (SPSS Inc, Chicago, Illinois, USA). All data were expressed as mean ± standard deviation or percentage. Comparisons between 2 groups were determined by the independent Student t test for continuous variables or the Pearson chi-square test for categorical variables, as appropriate. Survival analysis was assessed using a Kaplan-Meier analysis, with the significance based on the log-rank test. Multiple regression analysis was carried out using Cox proportional hazard regression analysis. A 2-sided P value < 0.05 was considered statistically significant.
Results
A total of 5965 newly diagnosed sleep apnea patients (mean age ± standard deviation, 45.22 ± 17.62 years) were identified from the 1 000 000 sampling cohort data set between January 1997 and December 2007. Another 29 669 (nearly 5 for every patient in the sleep apnea group) subjects without sleep apnea (mean age ± standard deviation, 45.15 ± 17.88 years) were matched for age, gender, and comorbidities to serve as the control group. The demographic parameters of study subjects are listed on Table 1 . Most enrollees in both groups (96.13% in the sleep apnea cohort and 96.17% in the control group) remained active and were followed through the end of study ( Figure 1 ).
| Sleep Apnea (n = 5965) | Control (n = 29 669) | P Value | |
|---|---|---|---|
| Age (y) | 45.22 ± 17.62 | 45.15 ± 17.88 | .804 a |
| Male (%) | 3721 (62.38) | 18 494 (62.33) | .958 |
| Follow-up (y) | 3.31 ± 2.41 | 3.81 ± 2.41 | <.001 a |
| Comorbidities (%) | |||
| Hypertension | 2024 (33.93) | 10 063 (33.92) | .996 |
| Diabetes mellitus | 1065 (17.85) | 5239 (17.66) | .731 |
| Coronary artery disease | 1313 (22.01) | 6481 (21.84) | .789 |
| Glaucoma | 261 (4.38) | 1212 (4.09) | .321 |
| Chronic kidney disease | 627 (10.51) | 3052 (10.29) | .619 |
| COPD | 1388 (23.27) | 6872 (23.16) | .872 |
| Asthma | 1003 (16.81) | 4940 (16.65) | .771 |
| Arrhythmia | 1166 (19.55) | 5738 (19.34) | .725 |
| Ischemic stroke | 377 (6.32) | 1809 (6.10) | .532 |
| Hyperlipidemia | 1695 (28.4) | 5232 (17.6) | <.001 |
| Development of RVO | 13 (0.22%) | 39 (0.13%) | .048 b |
During a follow-up period of 3.72 ± 2.42 years, there was a significantly higher incidence of RVO among sleep apnea patients as compared with the control group (13 [0.22%] vs 39 [0.13%]; P = 0.048, log-rank test; see Figure 2 ) . Incidence of RVO in the sleep apnea and control groups was 0.066%/year and 0.035%/year, respectively. After adjusting for age, sex, and comorbidities, increasing age (hazard ratio [HR], 1.04; 95% confidence interval [CI], 1.02 to 1.06; P < .001), hypertension (HR, 3.16; 95% CI, 1.48 to 6.73; P = .003), glaucoma (HR, 5.30; 95% CI, 2.80 to 10.00; P < .001), and sleep apnea (HR, 1.94; 95% CI, 1.03 to 3.65; P = .041) were associated independently with RVO development ( Table 2 ).
| Hazard Ratio | 95% Confidence Interval for Hazard Ratio | P Value | |
|---|---|---|---|
| Sleep apnea | 1.94 | 1.03 to 3.65 | .041 |
| Age | 1.04 | 1.02 to 1.06 | <.001 |
| Male sex | 1.09 | 0.62 to 1.91 | .776 |
| Hypertension | 3.16 | 1.48 to 6.73 | .003 |
| Diabetes mellitus | 0.71 | 0.37 to 1.35 | .295 |
| Coronary artery disease | 1.07 | 0.56 to 2.05 | .838 |
| Glaucoma | 5.30 | 2.80 to 10.00 | <.001 |
| Chronic kidney disease | 1.22 | 0.59 to 2.52 | .582 |
| COPD | 1.32 | 0.70 to 2.46 | .391 |
| Asthma | 0.77 | 0.38 to 1.58 | .478 |
| Arrhythmia | 1.27 | 0.68 to 2.37 | .459 |
| Ischemic stroke | 0.66 | 0.27 to 1.61 | .365 |
| Hyperlipidemia | 0.88 | 0.46 to 1.70 | .711 |
Results
A total of 5965 newly diagnosed sleep apnea patients (mean age ± standard deviation, 45.22 ± 17.62 years) were identified from the 1 000 000 sampling cohort data set between January 1997 and December 2007. Another 29 669 (nearly 5 for every patient in the sleep apnea group) subjects without sleep apnea (mean age ± standard deviation, 45.15 ± 17.88 years) were matched for age, gender, and comorbidities to serve as the control group. The demographic parameters of study subjects are listed on Table 1 . Most enrollees in both groups (96.13% in the sleep apnea cohort and 96.17% in the control group) remained active and were followed through the end of study ( Figure 1 ).



