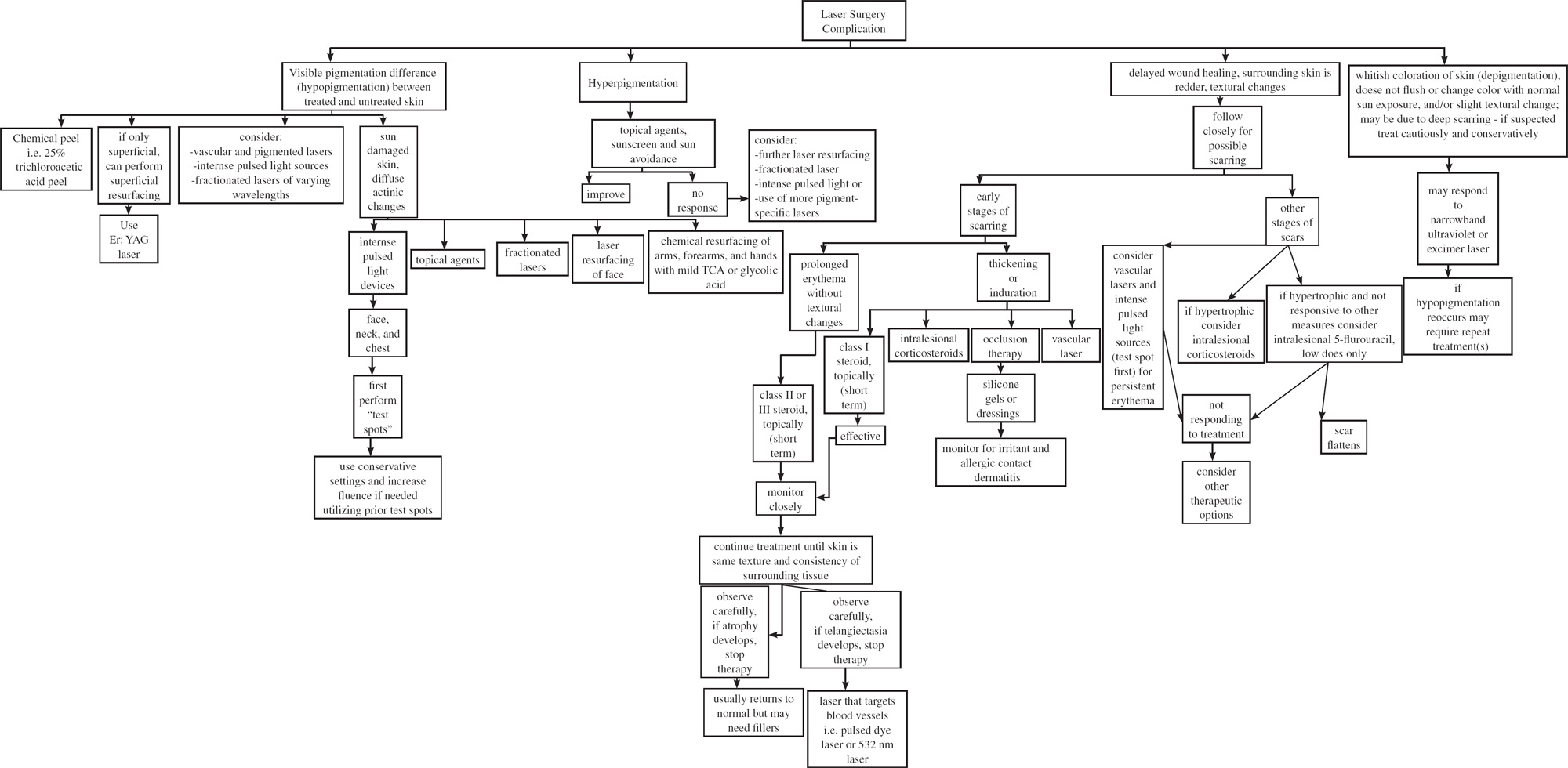
38 Skin Resurfacing: Laser Revision Surgery Complications following ablative laser and other resurfacing procedures are relatively infrequent, but when they do occur, they need to be treated quickly and efficiently to minimize patient anxiety and long-term morbidity. Obviously, patient selection, surgical management, and postoperative care are necessary to help prevent complications, but even in the best of cases, complications do occur. In this chapter, we will try to address some of the more commonly seen complications and discuss options for their treatment. An updated approach to revision is necessary, and the surgeon must be diligent in keeping up with the latest technologies. Lightening of the skin is desirable for most patients undergoing facial rejuvenation. Mottled hyperpigmentation, lentigines, and the sallow yellow tones that photodamaged skin develops are lessened or removed with the various resurfacing techniques, including carbon dioxide (CO2) laser, erbium:yttrium aluminum garnet (Erb:YAG) laser, and other resurfacing, as well as medium and deep chemical peels and dermabrasion. Some patients will present just for treatment of lentigines and other pigmentary problems. Patients who undergo resurfacing of cosmetic units, such as the perioral area or periocular area, may exhibit a lighter noticeable difference between the “new” treated skin and the untreated skin that exhibits the various dyschromias associated with photoaging. In these cases, treating the remaining skin will lighten the hyperpigmentation and help to blend in the differences. Although topical agents such as retinoids and hydroquinones can be used, visible results take months and are not practical for most patients. Although nonablative technology can also yield improvements, revision resurfacing is the most efficient way to improve a patient’s appearance in these cases and to blend in pigmentary alteration left by the resurfacing. Depending on the severity, a chemical peel such as a Jessner’s/35% trichloroacetic acid (TCA) peel may be sufficient, or laser resurfacing can be performed. When superficial resurfacing is all that is required for blending, the Er:YAG laser is an effective device. This superficial erbium resurfacing typically has a brief associated recovery period. Postresurfacing, pinkness resolves and reepithelialization occurs in a few days to a week. The goal of this procedure is to remove the epidermis; depending on the laser, one or two passes may be all that are required. This usually heals rapidly and with minimum risks. Other options that may be useful include the newer vascular and pigmented lasers, as well as intense pulsed light sources and fractionated lasers of varying wavelengths. These are discussed in more detail in the following sections. The goal is to improve the appearance of the skin and blend it with adjacent untreated skin. In the very sun-damaged patient, it may be difficult to find a good stopping point, due to diffuse actinic changes. In these instances, treating the full face may only accentuate the neck’s discoloration. If rejuvenation of the neck is performed, it may accentuate the chest’s skin changes. With some of the more recent technology and techniques, skin can be treated in the neck and chest area, extending onto the breast, but there is a risk that this may accentuate the actinic changes of the arms and forearms. In these patients, a combination of modalities can be used: topical agents as described above for the entire area, laser resurfacing of the face, lighter resurfacing of the neck and chest (we generally use chemical agents such as 20 to 30% TCA or 70% glycolic acid, but Er:YAG laser resurfacing has been used successfully by some physicians), and chemical resurfacing of the arms, forearms, and hands with 20 to 30% TCA or 70% glycolic acid (Fig. 38.1). More recently a shorter wavelength fractionated laser has become available (Microspot VariLite, Iridex, Mountain View, California) that can be judiciously used to treat chest lentigines and vascular lesions. As there is a paucity of sebaceous glands and adnexal structures in the chest and neck compared with the face, any procedure, including resurfacing, should be performed cautiously to help prevent scarring.1,2 Another option is the use of nonablative intense pulsed light devices for a “photofacial” technique. To minimize complications, it is important to adjust the setting for each patient’s skin. One system, available through Lumenis (Santa Clara, California), uses a broad spectrum intense pulsed light source with changeable crystals attached to the handpiece to filter out undesirable wavelengths. Similar devices are available from other manufacturers. This modality has been applied to the face, neck, chest, and upper extremities. Numerous treatment sessions are required but are generally well tolerated, with little to no “healing time” for the patients. The parameters used must be adjusted for each patient’s skin. As described, the neck has fewer pilosebaceous units and would generally be treated more conservatively, using lower fluences. Furthermore, the lower neck has a greater tendency to scar, and if treated, an even more conservative setting should be used. Decision tree for laser surgery complication Figure 38.1 (A) A 33-year-old woman approximately 1 year after an erbium: yttrium aluminum garnet (Er:YAG) laser resurfacing of the periocular area resulting in local hypopigmentation and accentuation of her melasma and surrounding facial hyperpigmentation. She had been treated with tretinoin solution and an unknown “bleaching” agent at the time of consultation. (B) Nine months after the use of tretinoin cream, hydroquinone, sunblock, and monthly glycolic acid peels 50 to 70%. A chilled gel is applied to the area prior to treatment. This helps to protect and cool the epidermis during the treatment. It is important that the operator carefully place the filters to avoid overlapping but also to prevent skipped areas or “footprinting.” These types of systems have a fairly high learning curve for the surgeon. This is particularly the case as there are different parameters that can be changed depending on the skin type, what is being treated, and individual patient variability. These devices have computer settings to assist in selecting the optimal parameters. Performing “test spots” can be useful before treating an entire area. Depending on the patient’s response during successive treatment sessions, deeper wavelengths may be chosen, and fluences can be increased. The 532 nm wavelength of the VariLite laser (Iridex, Mountain View) with a scanner can also be used to achieve a “photofacial” effect. This also requires a few treatments and the use of cooling gel. Typically for a “photofacial,” a scanner coverage of 45% is used with a thin layer of protective cooling gel. Before each treatment test spots should be performed to determine the optimum settings. After treatment some patients will have mild pinkness for up to a few hours. One of us (PJC) has been pleased with the results of this technique. True depigmentation of the skin following laser resurfacing is more difficult to treat than the relative pseudohypopigmentation described above. The skin acquires a whitish coloration and does not flush or change color with normal sun exposure. A slight textural change can even be noted at times such that the patient will complain that makeup does not “stick” to the skin well or does not last as long as the makeup applied to other areas. It can occur after any form of resurfacing, but it has been our experience that it is more commonly encountered with CO2 laser resurfacing and is less commonly seen following Er:YAG laser resurfacing. Considering the lower risk of complications and short recovery, the first author uses this laser more frequently than the resurfacing CO2 laser. When hypopigmented areas are evaluated histologically, there has been a varying quantity of epidermal melanin present. Typically, residual epidermal melanocytes are present, indicating that repigmentation should be possible. Mild perivascular inflammation has been noted in 50% of biopsies, and superficial dermal fibrosis was present in all biopsies.3 This suggests that the pathogenesis of the laser-induced hypopigmentation may be related to a suppression of melanogenesis and not destruction of the melanocytes. Grimes and colleagues have reported the successful treatment of hypopigmentation following CO2 laser resurfacing using topical photochemotherapy twice weekly.3 Seven patients were treated with topical 8-methoxpsoralen (0.001%) in conjunction with ultraviolet A (UVA) therapy. Moderate to excellent repigmentation was demonstrated in 71% of the patients. This pilot study suggests that phototherapy may be a viable therapy of laser-induced hypopigmentation. Using the same reasoning, narrowband ultraviolet B (UVB) and the excimer laser may both be effective. Narrowband UVB, which emits 311 to 312 nm, has been reported to be efficacious for vitiligo and may have fewer adverse effects than topical phototherapy.4,5 At the time of this writing, there are no published reports on narrowband ultraviolet therapy treating laser-induced hypopigmentation. The excimer laser emits 308 nm wavelength and can be targeted to a given site. Friedman and Geronemus have reported two patients who were treated for laser-induced leukoderma using the excimer laser.6 The first patient had > 75% improvement in pigmentation and the second patient had ~50% improvement after 10 treatment sessions to her upper lip. The average cumulative UVB dose was 1750 mJ/cm2
Pigmentary Abnormalities
Hypopigmentation

Depigmentation
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Skin Resurfacing: Laser Revision Surgery