Lid skin is quite thin. III. Expression of immunohistochemical markers for cytokeratins, mucin, and stem cells varies considerably among the various epithelia at the mucocutaneous junction of the eyelid. B. Reactivity also is found for MUC1 and MUC4 but not for MUC5AC. The dermis is sparse, composed of delicate collagen fibrils, and contains the vasculature and epidermal appendages, sebaceous glands, apocrine and eccrine sweat glands, and hair complexes. The subcutaneous layer is mostly composed of adipose tissue. I. The stratum corneum (keratin layer) is thickened. Hyperkeratosis means “increased scale” and includes both orthokeratosis and parakeratosis. In orthokeratosis, a thick granular layer is found because the epidermal cells slowly migrate upward; when the migration upward is rapid, no granular cells are seen and parakeratosis results. Orthokeratosis is hyperkeratosis composed of cells that have complete keratinization and no nuclear remnants, whereas parakeratosis is hyperkeratosis that shows incomplete keratinization in which nuclei are retained in the cells of the stratum corneum. Orthokeratosis and parakeratosis often exist in the same lesion (Fig. 6.3A). I. Dyskeratosis is keratinization of individual cells within the stratum spinosum, where the cells are not normally keratinized (Fig. 6.4A; see Fig. 7.18). The keratinizing cells show abundant pink (eosinophilic) cytoplasm and small, normal-appearing nuclei. I. Atrophy (see subsection Atrophy later, under Aging, and Fig. 6.8) is (1) thinning of the epidermis; (2) smoothing or diminution (effacement) of rete ridges (“pegs”); (3) disorder of epidermal architecture; (4) diminution or loss of epidermal appendages such as hair; and (5) alterations of the collagen and elastic dermal fibers. I. An atypical cell (see Fig. 6.4B) is one in which the normal nucleus-to-cytoplasm ratio is altered in favor of the nucleus, which stains darker than normal (hyperchromasia), may show an abnormal configuration (giant form or multinucleated form), may have an abnormal nuclear configuration (e.g., indented, cerebriform, multinucleated), or may contain an abnormal mitotic figure (e.g., tripolar metaphase). If sufficiently atypical, according to generally accepted criteria, the cell may be classified as cancerous. See Chapter 14. I. Phakomatous choristoma (Fig. 6.6) is a rare, congenital, choristomatous tumor (i.e., a tumor of tissue not normally found in the area) of lenticular anlage, usually involving the inner aspect of the lower lid. III. Neurocutaneous pattern syndromes are a group of disorders characterized by congenital abnormalities involving both the skin and the nervous system for which no identifiable cause has been isolated. Examples are encephalocraniocutaneous lipomatosis, oculocerebrocutaneous syndrome, and linear nevus sebaceous syndrome. IV. Caliber persistent artery refers to a large-caliber artery that is present adjacent to an epithelial or mucosal surface. Microblepharon is a rare condition in which the lids are usually normally formed but shortened; the shortening results in incomplete lid closure. A clinically and histologically normal caruncle may be present in the tarsal area of the lower lid. I. Ichthyosis (Fig. 6.7) can be divided into four types: A. Autosomal-dominant ichthyosis vulgaris (onset usually in first year of life) C. X-linked recessive ichthyosis vulgaris [the rarest type (Xp22.32), onset at 1–3 weeks] D. Autosomal-recessive ichthyosis congenita with a severe harlequin type and a less severe lamellar type (onset at birth) 2. Intact cross-linkage of cornified cell envelopes is required for epidermal tissue homeostasis. II. All types have in common dryness of the skin with variable amounts of profuse scaling. Only in the autosomal-recessive type do ectropion of the lids and conjunctival changes develop. III. Cicatricial ectropion is a common finding in recessive ichthyosis congenita. V. Histologically, the epidermis is thickened and covered by a thick, dense, orthokeratotic scale. See subsection Atrophy, earlier, under Terminology.
Skin and Lacrimal Drainage System
Skin
Normal Anatomy (Figs. 6.1 and 6.2)
Epidermis
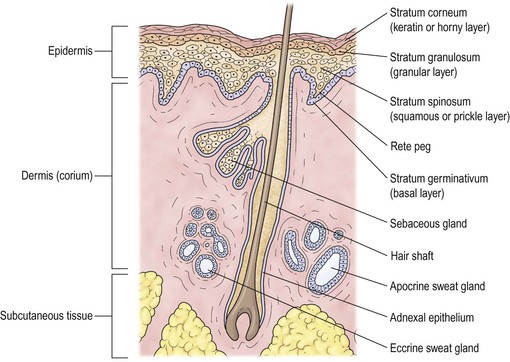
Dermis
Subcutaneous Tissue
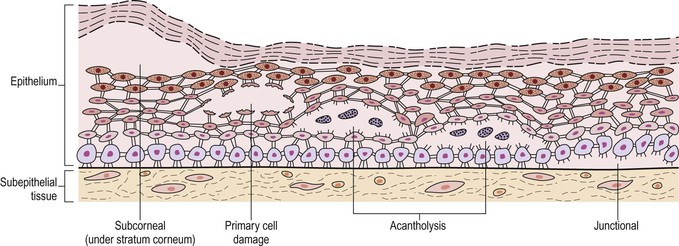
Terminology
Orthokeratosis and Parakeratosis
Dyskeratosis
Atrophy
Atypical Cell
Congenital Abnormalities
Dermoid and Epidermoid Cysts
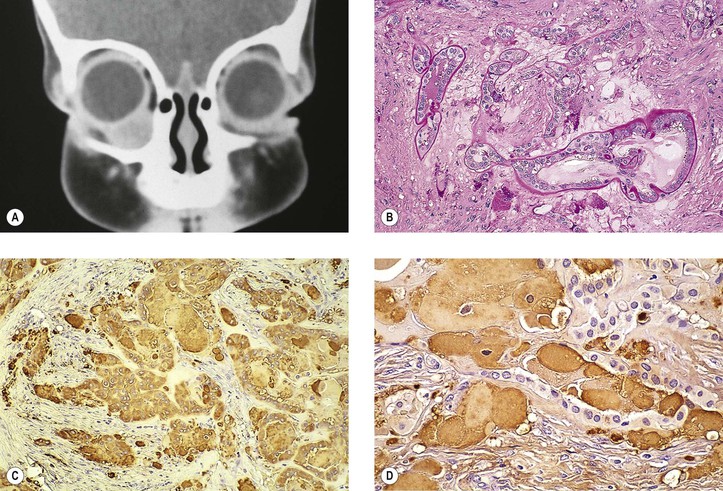
Phakomatous Choristoma
Miscellaneous Choristomas and Hamartomas
Microblepharon
Ectopic Caruncle
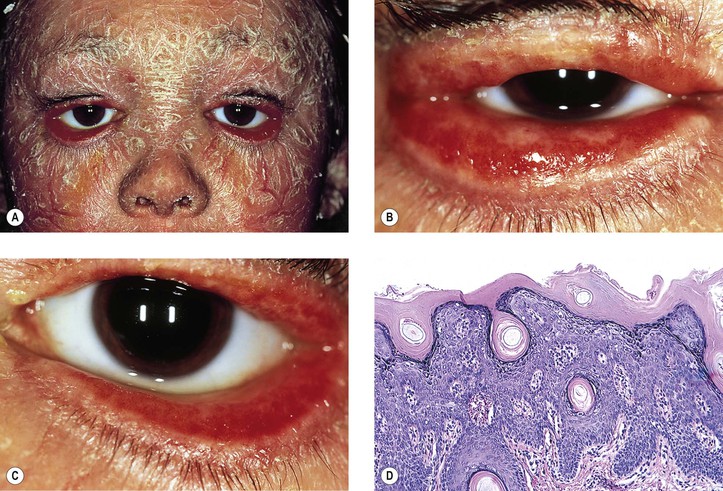
Ichthyosis Congenita
Aging
Atrophy
Skin and Lacrimal Drainage System
6
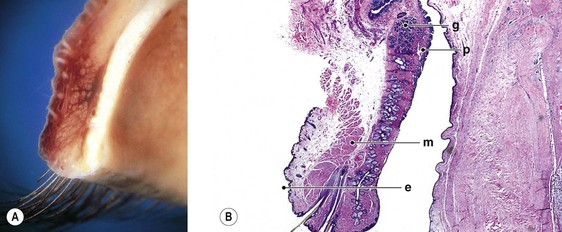
Fig. 6.2 Normal anatomy. A, Cross-section of the eyelid shows the inner white tarsal plate, the middle layers of muscle fibers, and the surface epithelium. Note the cilia coming out of the lid margin inferiorly. B, Histologic section shows the inner tarsal plate (p) containing the meibomian glands, the middle muscular bundles (m), and the surface epithelium (e). The cilia exit from the middle portion of the lid margin inferiorly. Apocrine sweat glands, eccrine sweat glands, sebaceous glands of Zeis, and hair follicles of the surface lanugo hairs are also seen in the lids (see also Figs. 1.27C and 7.1) (g, accessory lacrimal glands). (A, Courtesy of Dr. RC Eagle, Jr.)
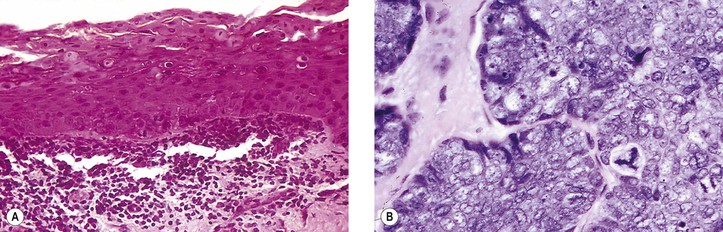
Fig. 6.4 Dyskeratosis and atypical cells. A, In this case of hereditary benign intraepithelial dyskeratosis, keratinization of individual cells is present in the stratum spinosum (squamous or prickle-cell layer)—see also Fig. 7.18B. B, In this sebaceous gland carcinoma, many atypical cells are seen, including a tripolar mitotic figure.