Purpose
To evaluate the safety and efficacy of topical bevacizumab in the treatment of corneal neovascularization.
Design
Prospective, nonrandomized, interventional case series.
Methods
setting: Institutional, multicenter clinical trial. study population: Twenty eyes from 20 patients with stable corneal neovascularization. intervention procedures: Patients were treated with topical 1.0% bevacizumab for 3 weeks and were monitored for a total of 24 weeks. main outcome measures: Primary outcome measures included: neovascular area, defined as the area of the corneal vessels themselves; vessel caliber, defined as the mean corneal vessel diameter; and invasion area, defined as the fraction of the total cornea into which the vessels extended. The occurrence of ocular and systemic adverse events was monitored closely.
Results
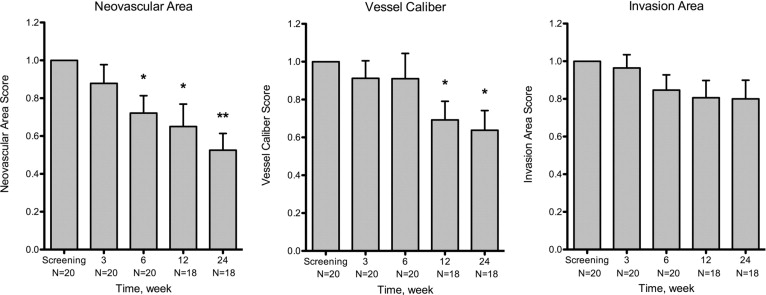
As compared with the baseline visit, patients exhibited a statistically significant improvement in neovascular area by week 6 ( P = .007) and in vessel caliber by week 12 ( P = .006). At the final visit, neovascular area, vessel caliber, and invasion area were reduced by 47.5%, 36.2%, and 20%, respectively. The decreases in neovascular area and vessel caliber were statistically significant ( P < .001 and P = .003, respectively); however, the reduction in invasion area did not reach statistical significance ( P = .06). There were no significant changes in the secondary outcomes, and there were no adverse events.
Conclusions
Short-term topical bevacizumab treatment reduced the extent of stable corneal neovascularization as measured by neovascular area and vessel caliber with no associated adverse events. Interestingly, the degree of treatment efficacy was inversely proportional to the baseline invasion area.
The healthy cornea is a unique tissue devoid of blood and lymphatic vessels. This feature is necessary for the maintenance of corneal transparency and visual acuity. Corneal neovascularization (CNV) can result from a variety of insults, including corneal infection, inflammation, trauma, degeneration, ischemia, and the loss of limbal stem cells. CNV is a devastating complication of the most common infectious causes of blindness in developed (herpetic keratitis) and developing (trachoma) countries. The presence of corneal vessels can influence corneal inflammation, scarring, edema, and lipid deposition, all of which decrease corneal transparency. In the case of corneal transplantation, ocular immune privilege, which helps extend the survival of corneal allografts, can be abrogated by CNV. In fact, the presence of stromal vessels in the host cornea is one of the strongest risk factors for subsequent graft failure.
Angiogenesis is promoted by a complex array of microenvironmental changes that involve a diverse array of cellular and molecular mediators. Vascular endothelial growth factor (VEGF) is a key factor in the development of neovascularization. Corneal epithelial cells, vascular endothelial cells, macrophages, and fibroblasts can produce VEGF. The production of VEGF is elevated significantly in inflamed and vascularized corneas. Bevacizumab (Avastin; Genentech, South San Francisco, California, USA) is a humanized, full-length, monoclonal anti-VEGF antibody that functions by binding and neutralizing VEGF, thereby inhibiting angiogenesis. Bevacizumab was first approved by the United States Food and Drug Administration in 2004 for the treatment of metastatic colorectal cancer. Since then, bevacizumab has been used off label to treat numerous cancers and a variety of ocular conditions, including neovascular age-related macular degeneration, central retinal vein occlusion, proliferative diabetic retinopathy, iris neovascularization, pterygium, and CNV.
Preliminary results from our study of topical bevacizumab in the treatment of CNV were published in 2009. We reported a statistically significant improvement in several measures of CNV with no associated adverse events. However, the limited number of patients in that study precluded the achievement of definitive conclusions regarding the relationship between medication efficacy and clinical factors such as the extent of CNV. Several studies, in some cases involving prolonged treatment, have reported complications associated with the administration of topical bevacizumab that were not identified in our preliminary study, including spontaneous corneal epitheliopathy, stromal thinning, and corneal perforation. The present study was limited to cases of stable CNV to avoid conditions such as pre-existing corneal epitheliopathy that may be associated with adverse events; moreover, the exclusion of active CNV potentially reduced the confounding effects of active ocular surface inflammation. Herein, we present the results of a clinical trial involving 20 cases of stable CNV treated with topical bevacizumab. Furthermore, we investigated potential correlations between treatment response and factors such as the extent of CNV and underlying disease state.
Methods
Design
This was a prospective, open-label, multicenter, uncontrolled, single-group safety and efficacy study of bevacizumab administered topically to patients with CNV. Subjects were recruited and treated at either The Massachusetts Eye & Ear Infirmary, Boston, Massachusetts, or The Walter Reed Army Medical Center, Washington, DC.
Patient Selection
Male and female adult patients were considered for study inclusion if they exhibited clinically stable CNV that extended at least 2 mm beyond the limbus. Clinical stability was established using the following exclusion criteria: (1) current or recent (3 months) ocular infection, (2) ocular surgery on the study eye within the previous 3 months, (3) current or recent (3 months) contact lens use, and (4) a current or recent (3 months) persistent corneal epithelial defect (14 days in duration measuring more than 1 mm 2 ). Additional exclusion criteria for patient selection included: (1) age 75 years or older, (2) uncontrolled hypertension (systolic blood pressure ≥ 150 mm Hg or diastolic blood pressure ≥ 90 mm Hg), (3) history of a thromboembolic event, (4) diabetes mellitus, (5) coagulation abnormalities including the use of anticoagulation medications other than aspirin, (6) current or recent (≤ 1 mo) systemic corticosteroid therapy or periocular corticosteroid injection to the study eye, (7) recent (≤ 1 mo) change in dose or frequency of topical steroids or nonsteroidal anti-inflammatory agents, (8) ocular or periocular malignancy, (9) pregnant women, lactating women, or premenopausal women not using adequate contraception, (10) recent (≤ 3 mo) or planned surgery, or (11) investigational therapy or anti-VEGF treatment within the past 60 days. Only 1 eye from each patient was selected for inclusion in this study.
Medication
A solution of 1.0% bevacizumab was formulated by the pharmacy at Massachusetts Eye & Ear Infirmary. Commercially available bevacizumab (25 mg/mL) was diluted in 0.01% benzalkonium chloride (0.1 mg/mL, pH = 6.2) to a concentration of 10 mg/mL. Study medication was stored in sterile, light-protected dropper containers at 2 to 8 C (36 to 46 F).
Treatment Protocol
All patients were provided with a solution of 1.0% bevacizumab. Treatment was administered via topical ocular instillation either 2 (n = 5) or 4 (n = 15) times daily over a period of 3 weeks. Patients were instructed to continue their usual ophthalmic medication regimens. Punctal plugs were placed in the patients’ superior and inferior puncta for the duration of the treatment (3 weeks) to minimize systemic drug absorption. The duration of treatment was limited to 3 weeks to minimize potential complications associated with long-term bevacizumab therapy.
Follow-Up Protocol
Study appointments were held during weeks 1, 3, 6, 12, and 24. A detailed review of medical history and a complete ocular examination including Snellen visual acuity measurement, slit-lamp biomicroscopy, and central corneal thickness measurement were performed during each visit. Digital corneal photography was performed at the baseline visit and weeks 3, 6, 12, and 24. Blood pressure was monitored at all visits.
Safety Measures
The occurrence of ocular and systemic adverse events was monitored closely over the course of this study. Ocular adverse events were monitored through complete ocular examinations along with visual acuity measurement, intraocular pressure measurement, biomicroscopy, and corneal fluorescein staining. Systemic adverse events were identified through physical examinations, patient questioning, and blood pressure measurements carried out throughout the study period.
Efficacy Measures
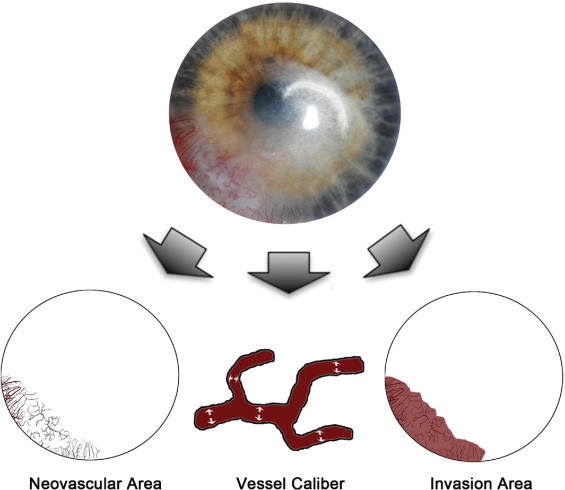
The primary measures of efficacy were the size and extent of CNV. The efficacy of bevacizumab in the treatment of CNV was evaluated by comparing corneal photographs obtained at baseline with corneal photographs obtained at follow-up visits. Secondary measures of efficacy included best-corrected visual acuity and central corneal thicknesses. Three primary metrics of CNV ( Figure 1 ) were investigated: (1) neovascular area, or the area of the corneal vessels when they are projected into the plane of a photograph; (2) vessel caliber, or the mean diameter of the corneal vessels; and (3) invasion area, or the fraction of the total corneal area into which the vessels extend. Digital slit-lamp corneal pictures were analyzed morphometrically using graphic editing software Photoshop CS2 (Adobe Systems, Inc, Berkeley, California, USA) and a program written in MATLAB (MathWorks, Inc, Natick, Massachusetts, USA). Through the use of the aforementioned software, we outlined the total corneal area and enhance blood vessel visibility with manual tracing. The nonvessel areas were excluded using a defined threshold, whereas the remaining neovascular area was pixelated for quantification. Vessel area was normalized to the entire corneal area to obtain a neovascular area score for each cornea. Vessel caliber was calculated using a computational technique that measures the largest diameter circle (centered at each pixel) inside of a blood vessel. The mean value across all pixels within the vessels was used as an estimate of the mean vessel caliber for a given image. Invasion area was quantified by marking the end of all vascular sprouts and connecting these marks to define the contour of the invasion area. The measured invasion area was normalized to the entire corneal area.
Statistical Analyses
All data are expressed as mean ± standard error of the mean. To quantify changes in CNV, measurements in each metric were obtained at each time point and were compared with their baseline values. A paired t test was performed using 2-sided alternatives to compare cohort scores for each metric. Other tests used in this study include: correlation test, 1-way analysis of variance (ANOVA), and the Bonferroni multiple comparison test. A P value of less than .05 was considered statistically significant. Statistics were calculated and graphs were composed using Microsoft Excel (Microsoft, Redmond, Washington, USA) and Prism 5 version 5.0c (GraphPad Software Inc, San Diego, California, USA).
Results
Demographics
Twenty eyes from 20 patients with stable CNV were included in this study. Demographic factors are listed in the Table , including each patient’s age, sex, and cause of CNV. There were 12 male and 8 female patients included in this study with an average age of 52.5 ± 3.3 years (n = 20), ranging from 24 to 75 years. Eighteen patients (90%) completed 24 weeks of follow-up, whereas 2 (10%) patients terminated their study visits at week 6 because nonstudy medication-related issues.
| Patient No. | Sex | Age (y) | Diagnosis | Dosage | Weeks of Follow-up | Additional Medications a |
|---|---|---|---|---|---|---|
| HSV/HZO keratitis | ||||||
| 1 | F | 50 | HSV keratitis | Twice daily | 6 | 1 |
| 2 | F | 51 | HSV keratitis | Twice daily | 24 | 2 |
| 3 | F | 65 | HZO keratitis | 4 times daily | 24 | 2, 3 |
| 4 | M | 40 | Underwent LASIK, HSV keratitis | 4 times daily | 24 | 2, 4 |
| 5 | F | 57 | HSV keratitis | 4 times daily | 24 | 4, 5 |
| 6 | M | 41 | HSV keratitis | 4 times daily | 6 | 6 |
| 7 b | M | 66 | HZO keratitis | 4 times daily | 24 | 6 |
| 8 b | M | 73 | HSV keratitis | 4 times daily | 24 | 1 |
| Keratoplasty/failed graft | ||||||
| 9 | F | 73 | Underwent PKP | Twice daily | 24 | 1, 3, 6 |
| 10 | M | 42 | Failed PKP | Twice daily | 24 | 1, 7 |
| 11 | F | 75 | Failed PKP | 4 times daily | 24 | 1, 6 |
| 12 | M | 55 | Failed PKP | 4 times daily | 24 | 2 |
| 13 | M | 39 | Failed PKP | 4 times daily | 24 | 2, 3, 6 |
| Limbal stem cell deficiency | ||||||
| 14 | F | 41 | LSCD | 4 times daily | 24 | 1, 6 |
| 15 | M | 39 | Underwent LASIK, partial LSCD | Twice daily | 24 | 2, 7 |
| 16 | F | 71 | LSCD | 4 times daily | 24 | None |
| 17 | M | 60 | LSCD | 4 times daily | 24 | 1 |
| Rosacea/dry eye | ||||||
| 18 | M | 24 | Rosacea, MGD | 4 times daily | 24 | 2, 7 |
| Pterygium | ||||||
| 19 | F | 48 | Underwent pterygium excision | 4 times daily | 24 | None |
| Corneal trauma | ||||||
| 20 b | M | 39 | Corneal laceration | 4 times daily | 24 | 5 |
a 1 = artificial tears; 2 = topical steroid; 3 = topical antibiotics; 4 = oral antiviral; 5 = topical antiglaucoma; 6 = topical cyclosporine; 7 = oral antibiotics.
Neovascular Area
There was a reduction in neovascular area by the end of the 3-week treatment period compared with baseline ( Figure 2 ), but this was not statistically significant (mean, −12.2 ± 9.9%; n = 20; P = .234). There was a statistically significant decrease by week 6 (mean, −27.9 ± 9.2%; n = 20; P = .007), which was 3 weeks after the termination of treatment. Statistically significant reductions in neovascular area were also observed at week 12 (mean, −35.0 ± 11.9%; n = 18; P = .009) and week 24 (mean, −47.5 ± 8.8%; n = 18; P < .001). Interestingly, there was a significant decrease in neovascular area at week 24 when compared with week 3 (mean, −28.5%; P = .002), indicating a delayed yet sustained medication response. The response rate, defined as the percentage of patients showing reduction in CNV when compared with baseline, was 65.0% (13 of 20 patients) for neovascular area at week 3, 85.0% (17 of 20 patients) at week 6, 77.8% (14 of 18 patients) at week 12, and 88.9% (16 of 18 patients) at week 24.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


