Chapter 25
SEVERE COMBINED ANTERIOR AND POSTERIOR SEGMENT TRAUMA

In dealing with the more severe eye injuries, it becomes less valuable to separate their classification and treatment artificially based on anatomical designations. Not surprisingly, the most serious injuries often involve both the anterior and posterior segments of the eye, crosscutting not only anatomical designations but also traditional ophthalmological disciplines (see Fig. 25–1). Corneal opacities/edema, hyphema, traumatic cataract, and choroidal and vitreous hemorrhages frequently obstruct visualization of the retina and may prevent safe and timely posterior segment reconstruction before the onset of severe scarring. Unfortunately, many of these severely injured eyes are still enucleated, without giving the surgeon a chance to visualize the postequatorial retina and the optic disk and thus accurately assess the viability of these vital tissues.
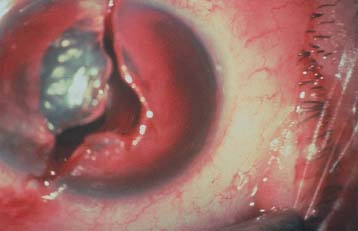
FIGURE 25–1 Open globe injury typical of trauma requiring TKP vitrectomy.
HISTORY
In 1981 the first TKP model (Landers-Foulksa) was introduced1 (see Table 25–l). This PMMA device permits pars plana vitrectomy for complete and timely treatment of severe posterior segment injuries in eyes with corneal opacification. A soft silicone rubber TKP model (Eckardt) was designed in 1987; this allowed a better view of the peripheral retina and, by having a shorter cylinder, was suitable for use even in phakic eyes.2,b
Since its original description, the Landers TKP has undergone a number of modifications, and it is now available with wide-field optics, a short cylinder, and a broad flange (see Fig. 25–2A and B).
PEARL… Both types of TKP are valuable as optical devices for exploration and reconstruction of the posterior segment of the globe in the presence of an opaque cornea. The results published in earlier series are encouraging.3,5
| Property | Landers* | Eckardt | ||
| Material | PMMA | Silicone rubber | ||
| Multiple use | Yes | Yes, but limited | ||
| Variable suture fixation | No | Yes | ||
| Wide-field optics available | Yes | Yes | ||
| Useful for phakic and pseudophakic eyes | Yes (short-cylinder version) | Yes | ||
| Useful with miotic pupil | Yes (standard cylinder version) | No; must use iris retractors | ||
| Available size (cylinder diameter in mm) | 7.2, 8.2 | 7 | ||
| Manufacturer | Wöhlk Contactlinsen, Kiel, Germany | Ocular Instruments, Bellevue, WA |
*The wide-field, short cylinder model
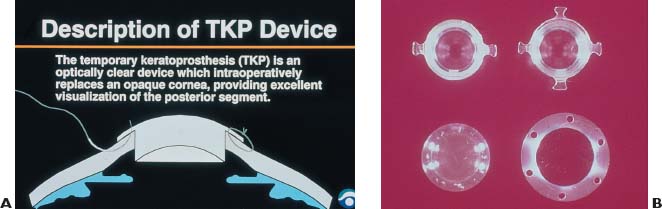
FIGURE 24–2 (A) TKP, schematic. (B) TKP models, clockwise from upper left: two-strut Landers-Foulks; four-strut Landers-Foulks; Eckardt; Landers wide-field.
CLINICAL RATIONALE FOR TKP USE
In very severely injured eyes, it is common for the surgeon to advise enucleation, instead of a direct inspection of the retina and optic disk. If, however, the retina and optic disk appear to be viable to the experienced trauma specialist, major intraocular reconstruction may be justified—provided the patients are adequately counseled regarding the relative risks and benefits and they desire the procedure (see Chapters 5, 7, and 8).
PEARL… The availability of even ambulatory vision as a “spare” to the better eye is of significant value to most patients.
PEARL… The TKP allows direct visual inspection of the postequatorial retina and optic disk by an experienced eye trauma surgeon so that a decision can be made whether to proceed with intraocular reconstructive efforts or, if appropriate, enucleation (see Chapter 8).
Alternatives to the TKP include:
• delayed surgery;
• inadequate surgery due to poor visualization;
• sequential surgery;
• no surgery; or
• endoscopic surgery.
None of these options allows timely, direct inspection and globe reconstruction utilizing all capabilities of modern vitreoretinal surgery while simultaneously restoring corneal transparency.
SURGICAL TECHNIQUE
In most cases, TKP vitrectomy is jointly performed by an anterior- and a posterior segment surgical team. The surgeons alternate responsibilities during the operation, each team adding its unique expertise to the procedure. In this way, the constellation of problems associated with severe combined anterior and posterior segment injuries can be addressed optimally while minimizing the potential complications associated with such a complex procedure.
We prefer general anesthesia as TKP vitrectomies tend to be lengthy and often unpredictable. There are, however, no absolute contraindications to local anesthesia if the surgeons feel that its benefits outweigh the potential complications or if the patient’s condition so requires (see Chapter 8).
Establishing the Surgical Field
The Posterior Segment Team
Typically, the vitreoretinal surgeon starts the procedure by opening the surgical field and preparing the eye for the intraocular reconstruction.
• A 360-degree conjunctival incision is made 2 to 3 mm posterior to the limbus to avoid disturbing the perilimbal stem cell population.
• The four rectus muscles are isolated on sutures to allow:
 control of the globe;
control of the globe;
 inspection of the external quadrants of the globe (if the primary repair was performed elsewhere, this may be the first time that the surgeon has the opportunity to visualize the extent and quality of the initial repair); and, if desired,
inspection of the external quadrants of the globe (if the primary repair was performed elsewhere, this may be the first time that the surgeon has the opportunity to visualize the extent and quality of the initial repair); and, if desired,
 scleral buckling later in the procedure.
scleral buckling later in the procedure.
• Primary wound repairs or surgical incisions are reinforced if found not to be watertight.
• The sclera is also inspected for any evidence of wounds that might have been missed at the time of primary repair; if present, these wounds are revised as necessary.
• Unless there is significant uncertainty regarding the anterior anatomical relationships, the infusion cannula is usually placed at this time.
• We generally initiate the intraocular segment of the surgery with an IOP of 25 mm Hg, set by a GFLI system.c The GFLI has the following advantages:
 allows accurate setting of the IOPd;
allows accurate setting of the IOPd;
 has a simple mechanism to change the IOP as operative conditions demand;
has a simple mechanism to change the IOP as operative conditions demand;
 the IOP change can be rapid if the need arises;
the IOP change can be rapid if the need arises;
 allows fast changes between fluid and gas environments as required throughout the operation; and
allows fast changes between fluid and gas environments as required throughout the operation; and
 has a digital IOP display, clearly visible to all operating room personnel even in the dark.
has a digital IOP display, clearly visible to all operating room personnel even in the dark.
• The cannula is typically placed in the inferotemporal quadrant, through the pars plana at 3.5 mm posterior to the limbus. Either a 4- or a 6-mm cannula can be used, similarly to standard vitrectomy cases. Typically, a special silicone oil infusion cannula set is chosen.
 Silicone oil cannula infusion sets differ from standard infusion sets; they have thicker walls, are less compliant than standard infusion tubing, and have a tubing that is firmly bonded to the cannula to reduce the risk of tubing disconnections or “blowouts.”
Silicone oil cannula infusion sets differ from standard infusion sets; they have thicker walls, are less compliant than standard infusion tubing, and have a tubing that is firmly bonded to the cannula to reduce the risk of tubing disconnections or “blowouts.”
• At this time, the posterior segment surgery team inspects the globe a last time prior to the placement of the TKP. The degree of corneal opacity is reassessed in cases where there is still some doubt about the possibility of performing a safe, effective, and complete posterior segment reconstructive procedure through the damaged cornea.
• Vitrectomy may be attempted with the option of converting to a TKP vitrectomy procedure if necessary.
PEARL… The infusion is not turned on until the cannula can actually be confirmed to be free within the vitreous cavity. Often this is not possible until after the TKP is actually placed.
PEARL… The authors use and recommend the GFLI for all vitrectomies.



