Purpose
To investigate graft survival and rejection following sequential bilateral corneal transplantation.
Design
Retrospective cohort study.
Methods
The study included patients with Fuchs endothelial dystrophy (FED), pseudophakic bullous keratopathy (PBK), or keratoconus who had undergone a penetrating keratoplasty (PK), endothelial keratoplasty (EK), or deep anterior lamellar keratoplasty (DALK) between 1999 and 2012. The main cohort included patients who had received a first transplant in both eyes for the same indication and a control cohort patients who had undergone a unilateral first corneal transplant. Main outcome measures were graft rejection or failure at 5 years.
Results
A total of 11 822 patients were included, of whom 9335 had a unilateral and 2487 bilateral corneal transplantation. For patients with FED ( P < .005) and KC ( P = .03) but not PBK ( P = .19), a transplant in the second eye was associated with a 50% reduction in risk of graft failure within 5 years in the first eye (FED: hazard ratio [HR] 0.47, 95% confidence interval [CI]: 0.34–0.64; KC: HR 0.50, 95% CI: 0.24–1.02). For FED this was dependent on the type of transplant (EK: HR 0.30, 95% CI: 0.17–0.52; PK: HR 0.61, 95% CI: 0.42–0.88). We found no association between a transplant in the second eye and a rejection episode in the first eye (KC P = .19, FED P = .39, PBK P = .19).
Conclusion
For FED and KC, a transplant in the second eye was associated with a reduced risk of graft failure in the first eye, independent of inter-transplant time. For FED this effect was pronounced following an EK in the first eye, where the risk of failure was reduced by 70%.
Corneal and kidney transplantation are the most commonly performed types of transplantation. The cornea differs from other tissues or organs in that it is a privileged site for transplantation owing to the absence of blood and lymphatic vessels, relative paucity of mature antigen-presenting cells, blood-eye barrier, and immunomodulatory factors within the eye. Despite this, corneal graft failure is significant, with an overall 5-year graft survival of 71% (95% confidence interval [CI]: 69%–73%). Corneal transplants fail predominantly from endothelial failure, as these cells do not divide and depend on survival of the donor endothelium. Corneal graft rejection and/or inflammation in the recipient are significant causes of endothelial failure. Many of the risk factors associated with rejection are well recognized, including young recipient age, vascularization, sex mismatch, and previous rejection episodes. In addition to donor- and recipient-related risk factors, graft survival is also dependent on the indication—for example, Fuchs endothelial dystrophy (FED), pseudophakic bullous keratopathy (PBK), and keratoconus (KC)—and the type of transplant—for example, penetrating keratoplasty (PK), endothelial keratoplasty (EK; Descemet-stripping endothelial keratoplasty [DSAEK] or Descemet membrane endothelial keratoplasty [DMEK]), or deep anterior lamellar keratoplasty (DALK).
Although there is a significant increase in the rate of rejection in an eye receiving a second corneal transplant, the effect of a transplant in the fellow or second eye on graft survival in either eye is unclear. This is an important question, because the common indications for corneal transplantation involve both eyes. Previous investigations have yielded conflicting results on the graft survival and rejection in patients undergoing bilateral corneal transplantation. The UK Transplant Registry offers an opportunity to address these issues, particularly as completion of transplant outcome data are a requirement for all transplants registered with National Healthy Service (NHS) Blood and Transplant. In order to investigate whether a transplant in the fellow eye was associated with graft survival and rejection in the first eye, graft failure and rejection in patients who have had sequential bilateral and unilateral corneal transplants were compared, taking into account the indication and type of transplant.
Methods
In a retrospective cohort study, data from the UK Transplant Registry were provided by and analyzed in collaboration with NHS Blood and Transplant, which provided institutional board approval. In the UK Transplant Registry, blanket informed consent is obtained at the time of corneal transplantation from all patients, allowing the use of registry data for scientific purposes. The study cohort comprised patients over 18 years in the UK with FED, PBK, and KC (which are the main indications for corneal transplantation ) who had undergone either a PK, EK, or DALK between April 1, 1999 and March 31, 2012. The bilateral cohort included all patients who had received a first transplant in both eyes, where the indication was the same in both eyes and the transplant in the second eye occurred within the follow-up period for the transplant in the first eye (maximum of 5 years) and before graft failure in the first eye. A control cohort included all patients who underwent unilateral first corneal transplant for the same indication during the same period. Patients who underwent a transplant in the second eye beyond the follow-up period for the first eye or after graft failure in the first eye were also included in the control cohort. Patient and outcome data were collected at the time of the transplant and then at 1 year, 2 years, and 5 years post-transplant. All data were obtained from the UK Transplant Registry for corneas supplied through the UK corneal transplant service (CTS) eye banks.
Post-transplant Endpoints
For the bilateral cohort, survival of the graft in either the first or second eye within 3 years of the time of transplant in the second eye was analyzed. In analyses comparing the bilateral and control cohorts, survival and time to rejection of the first eye graft within 5 years of the time of transplant in the first eye were the endpoints of interest. Survival times were censored for patients with a functioning graft at last follow-up. Time to rejection was censored for patients without rejection at last follow-up.
Analysis
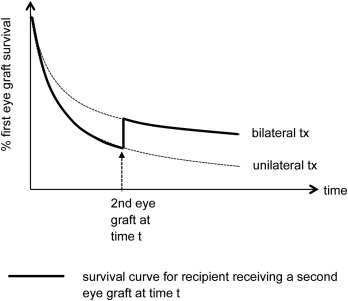
Recipient and transplant characteristics of the bilateral cohort were summarized as counts and percentages. For the bilateral cohort, the median time between transplants in the first and second eye was defined as the inter-transplant time (ITT) and compared across indications using the Kruskal-Wallis test. Kaplan-Meier estimates of first and second eye graft survival from time of second eye graft were compared across ITT categories (<1 year, 1–2 years, >2 years) for each indication using the log-rank test. The association between ITT and first and second eye graft survival from time of second eye graft was further investigated using Cox regression. Nonlinear associations between ITT and first and second eye graft survival were assessed using the likelihood ratio test, comparing a linear form of ITT with the categorical form of ITT. In analyses comparing the bilateral cohort and the control cohort, survival and rejection-free rates for the first eye graft at 5 years post-transplant were estimated using the Kaplan-Meier method. The association between receiving a graft in the second eye and survival and rejection of the first eye graft was investigated using Cox regression. Because it was not known if and when a recipient would receive a transplant in the fellow eye at the time of the transplant in the first eye, a time-dependent indicator variable that changed from 0 to 1 at the time of the transplant in the second eye was used in the model, as shown in Figure 1 . Regression analyses were performed separately for patients with FED, PBK, and KC, adjusting for the type of transplant (PK, DALK, and EK) as appropriate to that indication, low- or high-risk recipient (high risk defined as any ocular surface disease, corneal vascularization, or glaucoma at time of transplant), and, for KC and FED patients, postoperative intraocular surgery (predominantly cataract surgery) in either eye following the transplant prior to graft failure and/or rejection. Postoperative intraocular surgery was included as a time-dependent variable. Analyses were undertaken using SAS/STAT version 9.4 (SAS Institute Inc, Cary, North Carolina, USA).
Results
A total of 11 822 patients were included, of whom 2487 had undergone bilateral corneal transplantation within the study period. Of the 2487 patients with bilateral corneal transplants, 1584 (64%) had undergone transplants in both eyes within the follow-up period for the first eye and before graft failure in the first eye; 743 patients (30%) had a functioning graft in the first eye at last follow-up but received a transplant in the second eye beyond the known follow-up period for the first eye; 114 patients (5%) received a transplant in the second eye after having had a repeat transplant in the first eye; and 46 patients (2%) received a transplant in the second eye after graft failure in the first eye, but before or without a repeat transplant in the first eye. Therefore, 1584 patients were defined as bilateral recipients for the purpose of this study. Of these, the proportions receiving the same type of transplant in the second eye as in the first eye were as follows: EK, 98%, PK, 80%, and DALK, 78%. Follow-up data for the transplant in the second eye were missing for 59 patients (3.7%). For these recipients, only data for the transplant in the first eye were used. Recipient and transplant characteristics for the bilateral cohort are shown in Table 1 .
| Characteristic | Level | N (%) |
|---|---|---|
| Graft type | PK | 1093 (69) |
| DALK | 134 (8) | |
| EK | 357 (23) | |
| Indication | KC | 504 (32) |
| FED | 991 (63) | |
| PBK | 89 (6) | |
| Recipient sex | Male | 748 (47) |
| Female | 836 (53) | |
| Recipient age (y) | 19–40 | 439 (28) |
| 41–60 | 220 (14) | |
| 61–75 | 587 (37) | |
| >75 | 338 (21) | |
| HLA-matched | No | 1546 (98) |
| Yes | 38 (2) | |
| High-risk | No | 1123 (71) |
| Yes | 461 (29) | |
| Other intraocular surgeries at time of graft | No | 1071 (68) |
| Yes | 513 (32) | |
| Complications at time of graft | No | 1564 (99) |
| Yes | 20 (1) | |
| Postoperative surgery prior to graft failure | No | 1440 (91) |
| Yes | 144 (9) | |
| Postoperative surgery prior to rejection | No | 1451 (92) |
| Yes | 133 (8) | |
| Time between first eye and second eye graft (y) | <1 | 322 (20) |
| 1–2 | 587 (37) | |
| >2 | 675 (43) |
Median ITT was higher for patients with KC (median 734 days, interquartile range [IQR] 503–1110 days) than for those with FED (median 616 days, IQR 378–981 days) and lowest for PBK (median 535 days, IQR 322–823 days) ( P < .0005). We found no evidence of a nonlinear association between ITT and first and second eye graft survival for any indication ( P > .2 in all cases) and hence a continuous linear form of ITT was used in all regression models. Graft survival in the first eye at 3 years from transplant in the second eye was higher for patients with KC (97.9%, 95% CI: 95.6%–99.0%) than for those with FED (92.4%, 95% CI: 89.5%–94.5%) and lowest for patients with PBK (74.7%, 95% CI: 60.1%–84.7%) ( P < .0005). Importantly, however, within each indication first eye graft survival estimates were similar, regardless of ITT (KC P = .16, FED P = .25, PBK P = .17) ( Figure 2 ). After risk adjustment, we found no association between ITT and graft survival in the first eye (KC P = .14, FED P = .59, PBK P = .97) ( Table 2 ). Similar to the first eye, graft survival in the second eye at 3 years from transplant in the second eye was higher for patients with KC (94.6%, 95% CI: 91.8%–96.4%) than for those with FED (88.5%, 95% CI: 86.0%–90.6%) and lowest for those patients with PBK (75.3%, 95% CI: 61.4%–84.8%) ( P < .0005). Again, within each indication, estimates of graft survival in the second eye graft were similar, regardless of ITT (KC P = .80, FED P = .74, PBK P = .36). After risk adjustment, we found no association between ITT and graft survival in the second eye (KC P = .92, FED P = .07, PBK P = .38) ( Table 2 ).
| Parameter | Transplants (N) | Graft Failure (N) | Hazard Ratio (95% CI) for Each Year Increase in ITT | P Value |
|---|---|---|---|---|
| Risk of graft failure in the first eye | ||||
| KC a | 504 | 7 | 0.50 (0.19–1.31) | .14 |
| FED a | 991 | 40 | 1.11 (0.76–1.64) | .59 |
| PBK b | 89 | 15 | 0.99 (0.50–1.96) | .97 |
| Risk of graft failure in the second eye | ||||
| KC a | 489 | 22 | 1.02 (0.70–1.47) | .92 |
| FED a | 950 | 91 | 1.18 (0.99–1.40) | .07 |
| PBK b | 86 | 15 | 1.22 (0.79–1.87) | .38 |
a Adjusted for graft type, low or high risk, and postoperative surgery prior to failure.
For all 11 822 patients who received a first eye graft, the overall 5-year graft survival rates were 91% (95% CI: 90%–92%) for KC, 78% (95% CI: 76%–80%) for FED, and 53% (95% CI: 51%–56%) for PBK. The overall 5-year rejection-free rates were 83% (95% CI: 81%–84%) for KC, 87% (95% CI: 85%–88%) for FED, and 77% (95% CI: 75%–79%) for PBK. Analysis of first eye graft outcomes for the whole study cohort indicated that, for patients with FED and KC, the risk of graft failure within 5 years in the first eye for patients who received a transplant in the second eye was half that of patients who did not receive a transplant in the second eye (FED: hazard ratio [HR] 0.47, 95% CI: 0.34–0.64, P < .005; KC: HR 0.50, 95% CI: 0.24–1.02, P = .03) ( Table 3 ). By including an interaction term in each model (type of transplant in the first eye by second eye graft), we found that this effect was independent of the type of transplant in the first eye for KC ( P = .23) but not for FED ( P = .03, EK: HR 0.30, 95% CI: 0.17–0.52; PK: HR 0.61, 95% CI: 0.42–0.88). For patients with PBK we found no association between a transplant in the second eye and graft failure in the first eye, regardless of the type of transplant in the first eye (HR 0.69, 95% CI:0.42–1.14, P = .61). As an additional measure of how well the first eye graft was doing post-transplant, we also included post-transplant corrected logMAR visual acuity in the first eye as a time-varying covariate in each model. We still found that a transplant in the second eye was associated with a reduced risk of graft failure, although the confidence intervals are far wider owing to missing values of logMAR visual acuity (FED: HR 0.69, 95% CI: 0.45–1.04; KC: HR 0.49, 95% CI: 0.20–1.18; PBK: HR 0.76, 95% CI: 0.34–1.71). In addition, we found no association between a transplant in the second eye and the development of a rejection episode in the first eye, regardless of the type of transplant in the first eye (KC P = .48, FED P = .11, PBK P = .85) ( Table 3 ). There were only a few cases of graft failure or rejection within 5 years of transplant where the type of transplant in the second eye was different from that for the first eye (KC: graft failure, 2 cases, graft rejection, 13 cases; FED: graft failure, 6 cases, graft rejection, 9 cases; PBK: graft failure, 1 case, graft rejection, 0 cases), so we were not able to estimate the effect of type of transplant in the second eye.
| Parameter | Level (Baseline) | Transplants (N) | Events (N) | Hazard Ratio (95% CI) for Graft in the Second Eye Compared With No Graft | P Value |
|---|---|---|---|---|---|
| Risk of graft failure in the first eye | |||||
| KC: Graft in second eye a | No | 4104 | 285 | 1.00 (–) | |
| Yes | 504 | 7 | 0.50 (0.24–1.02) | .03 | |
| FED: Graft in second eye a | No | 2966 | 540 | 1.00 (–) | |
| Yes | 991 | 47 | 0.47 (0.34–0.64) | <.01 | |
| PBK: Graft in second eye b | No | 3168 | 984 | 1.00 (–) | |
| Yes | 89 | 15 | 0.69 (0.42–1.14) | .13 | |
| Risk of rejection in the first eye | |||||
| KC: Graft in second eye a | No | 4104 | 546 | 1.00 (–) | |
| Yes | 504 | 58 | 0.72 (0.43–1.20) | .19 | |
| FED: Graft in second eye a | No | 2966 | 277 | 1.00 (–) | |
| Yes | 991 | 78 | 0.85 (0.59–1.23) | .39 | |
| PBK: Graft in second eye b | No | 3168 | 466 | 1.00 (–) | |
| Yes | 89 | 11 | 0.55 (0.20–1.47) | .19 | |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


