Techniques used for the diagnoses and treatment of septal deformity vary according to indications for the procedure and surgeon preference. Septoplasty is commonly performed to treat septal deformity causing nasal airway obstruction. Various preoperative and intraoperative “pearls” that the authors have found to be helpful in treating septal deformity and nasal airway obstruction are discussed.
The predominant surgical treatment for obstructive deviation of the nasal septum during the first half of the twentieth century was to perform a submucous resection (SMR). The SMR was initially popularized by Killian and Freer in the early 1900s to allow for removal of bony and cartilaginous deformities of the nasal septum. During SMR, deformities of the dorsal and caudal portions of the septum are not addressed in order to prevent postoperative saddle nose deformities and a retracted columella. Often, the septal deformities are removed, and straight pieces of cartilage or bone are not replaced.
In 1948, Cottle and Loring published an article describing a new operative procedure on the nasal septum that allowed the surgeon to address deformities in all portions of the septum in addition to avoiding postoperative deformities. In that article, Cottle and Loring those researchers described the disadvantages of performing a Killian type incision near the mucocutaneous junction or more posterior. It is difficult to treat areas of obstruction located anterior to the Killian incision. They also described some disadvantages associated with bisecting the mucosal flaps, including the disruption of normal ciliary activity and interruption of the blood supply to the flap that feeds the replaced bone or cartilage.
Cottle and Loring described the importance of addressing all portions of the bony and cartilaginous septum that are deviated. They stated that one should not hesitate to remove all the bone or cartilage that interferes with the normal passage of air in the nose. Once the airway is improved, they recommend replacing trimmed, thinned, and straightened pieces of septum between the mucosal flaps. Placing these pieces of cartilage provides support and, more importantly, prevents postoperative scar formation. This reduces contracture and subsequent deformity.
General approach
The authors have found that caudal and dorsal septal deformities often contribute to the patient’s obstruction. For this reason, they believe that a hemitransfixion incision and the approach described by Cottle and Loring provide the best opportunity to treat deformities in these and other areas of the septum. They have also found it to be beneficial to preserve as much of the cartilaginous septum as possible and to replace excised portions with straightened septal grafts. They typically liberally excise bony irregularities, taking care to preserve the keystone area at the nasion.
The hemitransfixion incision and initial elevation of the mucoperichondrial flap are performed on the concave side of the cartilaginous septal deformity. The bony-cartilaginous junction is then separated, and mucoperiosteal flaps are raised bilaterally. The bony septum is then addressed. The authors attempt to treat the cartilaginous portion without raising the opposite mucosal flap. By elevating on the concave side, one can perform scoring maneuvers on the appropriate surface of the septal deformity. If scoring does not adequately treat the deformity, they move on to raise the contralateral flap and perform vertical slats or excision of portions of the cartilaginous septum. If the cartilaginous septum has a severe deformity or deviations in critical portions of the septum, they may perform explantation and reimplantation of the cartilage.
One of the most common cartilaginous septal deformities that the authors have encountered is that of an overly long quadrangular cartilage that is projected off of the maxillary crest in one side of the nasal cavity with subsequent bowing of the cartilage into the other side of the nose. This type of deformity can be treated by excising an inferior strip of the septum and placing the new inferior border on the maxillary crest.
Septal spurs, cartilaginous and bony, are also commonly encountered and are found to contribute to nasal obstruction. In this case, the authors often raise the mucosal flap on the side of the spur first. A tunnel is raised superior and inferior to the spur. The cartilaginous spur can then be separated from the septum and carefully freed from its lateral most attachments. Many times, the quadrangular cartilage and mucoperichondrial flap on the opposite side do not need to be violated. This provides the surgeon with the best opportunity to ensure that one of the flaps maintains its integrity and is not perforated. The bony or cartilaginous attachment can then be separated, and the bony septum can be addressed as usual.
In the upcoming sections, the authors describe some specific “pearls” that they have found helpful in treating patients with difficult-to-treat nasal septal deformities. They believe that the application of these pearls leads to increased satisfaction and decreased rates of revision surgery for patients.
Pearl 1: Don’t Miss The Nasal Valve
The anatomy, dysfunction, and treatment of the nasal valve have been well described. A recent study points out that even among otolaryngologists, however, there continues to be “uncertainty and unease of sorts in defining the nasal valve component regions.” In a recent study, the authors found that 51% of patients undergoing revision septoplasty required treatment of the nasal valve to correct their nasal airway obstruction. In contrast, only 4% of patients who underwent treatment of the valve during a primary septoplasty required revision surgery for nasal obstruction. They surmise that there are two main explanations for these data: (1) the surgeon is missing the contribution of the nasal valve before the primary surgery or (2) the patient develops narrowing of the valve over time.
In some instances, it is likely that both are contributing causes of the patient’s continued airway obstruction. Therefore, it is important assess the anatomy of the nasal valve to determine if there is dysfunction at the valve.
The internal nasal valve is bounded by the nasal septum, the caudal border of the upper lateral cartilage, and the lateral nasal wall at the level of the anterior surface of the inferior turbinate. Dysfunction of the internal valve may be attributable to collapse of the upper lateral cartilage toward the septum, dorsal deviation of the septum toward the valve, or a combination of both. Collapse of the caudal border of the upper lateral cartilage may be dynamic, static, or both. Determining the cause of the internal valve obstruction is necessary to determine the correct approach for treatment.
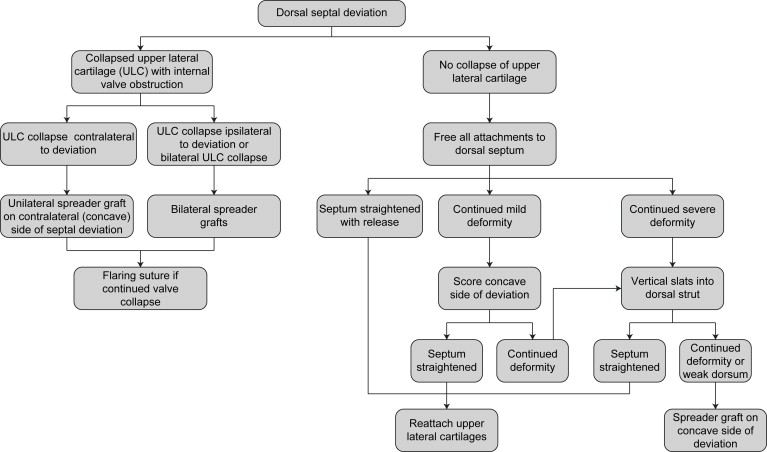
Static obstruction of the internal nasal valve attributable to collapsed upper lateral cartilage may be treated by placement of a spreader graft or flaring suture. In this study, the combination of flaring sutures and spreader grafts provided the greatest impact on the cross-sectional area of the nasal valve ( Fig. 1 ). Some patients have static obstruction attributable to a dorsal septal deviation at the location of the valve with or without collapse of the upper lateral cartilage as well. In these instances, the dorsal deflection must be addressed in addition to the upper lateral cartilage. This is described in further detail in the next section (pearl 2). These patients are often treated with a spreader graft to splint the dorsal septum and treat the valve. A flaring suture may be incorporated as well.
Dynamic collapse of the nasal sidewall can contribute to nasal obstruction as well. Dorsal or caudal deflections of the septum can often accentuate the obstruction caused by collapse of the sidewall. In these instances, one should treat the septal deflection in addition to the sidewall collapse. Collapse of the nasal sidewall or vestibule may be attributable to deformity in the area of the external valve or intervalve. The external valve deformity is rare, and treatment is directed at relieving the cause of cicatricial stenosis causing the deformity. The authors have found that dynamic valve obstruction is most frequently attributable to dysfunction at the intervalve area. The intervalve area is located at the caudal edge of the lateral crus, extending laterally toward the piriform aperture, including the area of the sesamoid cartilages. Collapse in this area often corresponds to a deep supra-alar crease and is treated by the placement of septal or auricular cartilage batten grafts. It is imperative that these grafts extend laterally over the piriform aperture to provide adequate support. In cases in which there is paradoxical concavity of the lateral crura, a lateral crural flip-flop graft may be performed. Lateral crural strut grafts or batten grafts may be used for recurvature of the lower lateral cartilage.
Spreader and batten grafts can be placed through endonasal and external approaches. The authors have found it best to place these grafts through an external approach. They believe this allows for better visualization in addition to precise and secure placement of the grafts. The external approach also allows the surgeon to place a flaring suture to improve the cross-sectional area of the internal valve further.
Pearl 2: Don’t Miss The Dorsal Deviation
When evaluating a patient with septal deviation, one’s attention is often drawn to deviations in the posterior or bony septum and to septal spurs. Caudal septal deformities are generally easy to diagnose yet more difficult to treat because of the importance of the support provided by the caudal portion of the septum. The authors have found, however, that deviations of the dorsal portion of the septum are often missed and frequently contribute significantly to the symptoms of nasal obstruction. It is difficult to know if dorsal deviations are noted but not treated because of the difficulty in accessing this area through traditional endonasal septoplasty approaches. Alternatively, deviations in this area may go unrecognized during the initial evaluation and treatment. Significant dorsal deviations of the septum can also result in significant deviations of the external appearance of the nose, resulting in a crooked nose deformity. As stated previously, dorsal deflections in the area of the caudal portion of the upper lateral cartilage accentuate nasal obstruction by contributing to internal nasal valve obstruction.
Although others have described treating dorsal irregularities through an endonasal or endoscopic approach, the authors have found it best to treat significant dorsal deformities through an external rhinoplasty approach. This allows the surgeon the opportunity to disarticulate the attachments of the mucoperichondrium and upper lateral cartilages to the dorsal portion of the septum and provides for complete and unobstructed access to the dorsal septum. It is also important to note that dorsal septal irregularities are not addressed through the SMR technique.
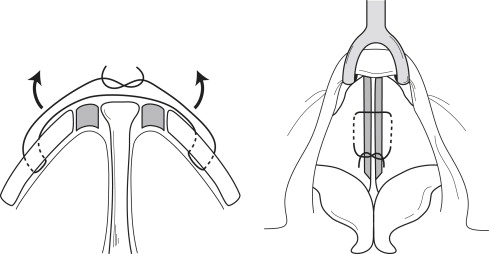
A chart summarizing the treatment of dorsal septal deviations causing nasal obstruction is shown in Fig. 2 . It is important first to free all the attachments from the dorsal septum. Freeing the dorsal septum occasionally allows the dorsal septum to straighten out, permitting the surgeon to reattach the upper lateral cartilages, resulting in adequate improvement of the airway and more a straightened appearance of the nasal dorsum. Often, the intrinsic deformity of the cartilage requires other maneuvers to straighten the septum appropriately. The concave portion of the deflection may be scored to release some of the intrinsic deformity that exists in the cartilage. In more severe cases, vertical slats may be placed into the dorsal strut; however, these should not extend up within 5 mm of the dorsal edge of the strut ( Fig. 3 ). If vertical slats are made into the dorsal strut, or if there is continued deformity, unilateral or bilateral spreader grafts should be placed to provide support and to act as a splint to straighten the dorsal deviation.