Nasal obstruction from a deviated septum is one of the more frequent complaints bringing patients into an otolaryngology office. Despite the significant number of septoplasties performed each year, complications after this procedure are relatively uncommon. Most complications result from inadequate surgical planning or poor technique and often can be prevented. Surgeons should discuss these risks with patients before surgery as part of the informed consent process. This article reviews how complications of septoplasty can occur, compromising the functional and aesthetic aspects of a patient’s life, and how attention to detail can reduce the risk for these complications. The septoplasty surgeon must be aware of all the possible complications that may arise so as to convey the benefits and risks of surgery effectively to prospective patients.
Although complications after septoplasty are rare, conservative approaches with proper preoperative diagnosis minimize such complications even further. The reported incidence of complications from septoplasty can range anywhere from 5% to 60%. Experience, meticulous surgical technique, and comprehensive preoperative planning are all necessary to limit complications. Additionally, the septoplasty surgeon must have a comprehensive understanding of the relevant anatomy, with a specific appreciation for high-risk areas. Although research by Bateman and colleagues has shown that no single surgical maneuver could be identified or associated with an increased risk for septoplasty complications, the need for meticulous surgical technique remains evident. Finally, the importance of experience cannot be understated because it combines methodic and systematic procedure with sound surgical judgment.
Preoperative planning and evaluation for septoplasty
With any surgical procedure, preoperative planning is essential, and septoplasty is no exception. Nasal obstruction from a deviated septum alone is not always an indication for immediate surgical intervention. Conservative medical therapies should always be attempted and documented before moving forward to the operating room. Significant anatomic obstructions, however, most often still require surgical management.
When evaluating a patient for septoplasty, extensive preoperative assessment is necessary, including a thorough documentation of the patient’s past medical and surgical history, allergies, and medications. Two of the more common complications from any surgery include bleeding and poor healing. Therefore, it is necessary to review all the patient’s preoperative medications, such as anticoagulation and herbal medicines, to reduce these risks. It is also critical to assess the patient’s history of tobacco use, because smoking cessation is advised for at least 2 to 4 weeks before and after surgery to avoid delayed nasal wound healing. Another consideration in the preoperative workup is a history of intranasal cocaine use. Cocaine users often have abnormalities in the mucoperichondrium leading to decreased vascularity of the septal cartilage secondary to the vasoconstrictive actions of the drug and irritative effects of other contaminating agents. Therefore, this puts these patients at risk for complications during septal surgical procedures.
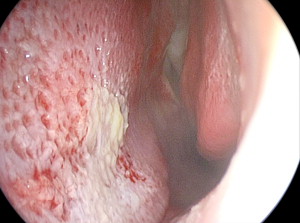
The presence of significant mucosal disease should raise awareness about several comorbid diseases that may compromise the results of a septoplasty. In fact, any pathologic changes to the septal mucosa on physical examination should arouse suspicion and be evaluated with a biopsy or blood serologies for autoimmune diseases and allergies. The most common changes include chronic inflammation, squamoproliferation, nonnecrotizing granulomas, foreign body giant cells, erosion, and ulceration ( Fig. 1 ).
An important step in planning for more complex septorhinoplasty cases includes preoperative photographs. It is crucial to have this confirmation for several reasons, including suitable surgical planning and preparedness, accurate postoperative assessment of aesthetic deformity secondary to the procedure, and protection in the event that litigation is brought about from an unhappy patient.
Finally, as with all procedures, proper informed consent and explanation are important, as is the need to have a thorough discussion of potential complications with the patient. All the following complications, including infection, bleeding, hematoma, septal perforation, scarring, sensory impairment, cerebrospinal fluid (CSF) leak, and aesthetic changes, should be specifically noted, in addition to the necessity of correcting them. The possibilities for revision surgery should also be explained at this time.
Anesthesia complications
Studies have shown that local anesthesia with sedation might lead to fewer complications for patients undergoing septoplasty than general anesthesia. General anesthesia was shown by Fedok and colleagues to require an intervention for bleeding or unintended hospital admission after surgery more frequently. In addition, postoperative nausea, emesis, and epistaxis rates were higher with general anesthesia, at 36%, 14%, and 3.6%, respectively, compared with local anesthesia with sedation at 8%, 3%, and 0%, respectively. Fedok and colleagues also showed that operating times, in addition to aggregate recovery times, were significantly lower when using local anesthesia with sedation over general anesthesia. When using local or monitored anesthesia care techniques, the authors have found that nasopharyngeal packs are an excellent adjuvant and prevent bleeding into the airway.
The use of topical and injectable anesthetics and vasoconstrictive agents has also been heavily debated, including the use of intraoperative cocaine. Although these drugs have many attractive properties, including rapid onset, prolonged duration of action, vasoconstriction, and decongestant effects, their complications have included mild anxiety, myocardial infarction, cerebral vascular accident, and death. Additionally, there are no present criteria to identify which patients may be at risk for these serious complications. It is important to remember the maximum dosing for each drug. The dose is additive; a 50% toxic dose of two separate drugs may become 100% toxic if they share similar properties. Accordingly, vigilant perioperative patient monitoring with blood pressure, pulse oximetry, and electrocardiography for quick intervention is necessary when using any of these anesthetic medications. Treatment initially includes oxygen, intravenous fluids, and removal of the cocaine-soaked pledgets. If cardiovascular alterations are noted, appropriate anesthesia care is necessary.
Anesthesia complications
Studies have shown that local anesthesia with sedation might lead to fewer complications for patients undergoing septoplasty than general anesthesia. General anesthesia was shown by Fedok and colleagues to require an intervention for bleeding or unintended hospital admission after surgery more frequently. In addition, postoperative nausea, emesis, and epistaxis rates were higher with general anesthesia, at 36%, 14%, and 3.6%, respectively, compared with local anesthesia with sedation at 8%, 3%, and 0%, respectively. Fedok and colleagues also showed that operating times, in addition to aggregate recovery times, were significantly lower when using local anesthesia with sedation over general anesthesia. When using local or monitored anesthesia care techniques, the authors have found that nasopharyngeal packs are an excellent adjuvant and prevent bleeding into the airway.
The use of topical and injectable anesthetics and vasoconstrictive agents has also been heavily debated, including the use of intraoperative cocaine. Although these drugs have many attractive properties, including rapid onset, prolonged duration of action, vasoconstriction, and decongestant effects, their complications have included mild anxiety, myocardial infarction, cerebral vascular accident, and death. Additionally, there are no present criteria to identify which patients may be at risk for these serious complications. It is important to remember the maximum dosing for each drug. The dose is additive; a 50% toxic dose of two separate drugs may become 100% toxic if they share similar properties. Accordingly, vigilant perioperative patient monitoring with blood pressure, pulse oximetry, and electrocardiography for quick intervention is necessary when using any of these anesthetic medications. Treatment initially includes oxygen, intravenous fluids, and removal of the cocaine-soaked pledgets. If cardiovascular alterations are noted, appropriate anesthesia care is necessary.
Functional complications
The occurrence of septoplasty complications can be separated temporally. They may be seen at the start of surgery and extend well beyond the completion of the healing phase. Following this time line, the authors review the most common complications.
Hemorrhage: Early
Bleeding or hemorrhage is one of the more common complications of septoplasty, usually occurring during surgery or immediately after surgery. When performing septoplasty surgery, it is important to tell all patients to expect 1 to 2 days of mild oozing after surgery.
True hemorrhage as a result of septoplasty has been reported at a rate of 6% to 13.4%, sometimes requiring admission and overnight observation. Acute bleeding during nasal surgery most frequently occurs as a result of poor injection technique or inadvertent mucosal trauma during flap elevation. To prevent bleeding from inadequate injection of local anesthesia, initial topical decongestion with oxymetazoline or cocaine for 5 to 10 minutes before making an incision not only improves visibility but offers the surgeon an opportunity to discern inflammatory mucosal disease from true anatomic septal irregularities. It is beneficial to inject the area in which the incisions are to be made and the important areas of vessel origins (dorsal septum, posterior bony septum, along the nasal floor, and at the anterior nasal spine) adequately. A total of 5 to 6 mL of local anesthesia is typically required for an adequate septal injection when adequate time for vasoconstriction is provided. Proper injections hydrodissect the mucoperichondrium off of the septal cartilage, aiding in flap elevation. In cases of “traumatic” noses or nasal septal fractures, hydrodissection may not work as well and multiple injection sites may help to minimize bleeding.
In terms of traumatic causes of bleeding with septoplasty, in addition to poor technique and accidental mucosal trauma with the septal needle during closure, concomitant intraoperative treatment of turbinate disease is suspected to be the most common cause of postoperative bleeding. The most common source of postoperative bleeding seems to be from the turbinate incision site for inferior turbinectomies. Given their vascularity, it is important to inject the head of each inferior turbinate with approximately 1 mL of local anesthesia 5 to 10 minutes before turbinectomy. Additionally, submucosal resection of the inferior turbinates with a microdebrider is a nice technique that not only allows for a quicker recovery but minimizes mucosal trauma compared with standard turbinate resection followed by cauterization. After the turbinectomy, oxymetazoline-soaked pledgets can be packed against the head of the turbinate for compression to limit bleeding further. They are then removed after extubation to avoid any bleeding at that time. It is always important to secure the pledget strings to avoid accidental aspiration.
There are many methods to prevent significant hemorrhage from occurring after a septoplasty. Although extensive intranasal cautery often tends to lengthen the healing process and the patient’s return to normal function, the use of a fibrin sealant may be an acceptable alternative. Fibrin sealant is a formulation based on a concentrate of human clottable proteins and a highly purified human thrombin. The amount of sealant required truly depends on the area of tissue to be treated. Vaiman and colleagues have shown that fibrin sealant, administered by aerosol spray in endonasal surgery, is more effective and convenient than nasal packing. The sealant facilitates hemostasis and prevents or reduces postoperative bleeding and oozing during surgical procedures. Also, as a human blood product, it stimulates normal wound healing of the operated area. No special treatment is required with the use of fibrin sealant, there is no danger of aspiration, and no antibiotics are necessary because there is no foreign object inserted into the nasal cavity. Vaiman and colleagues have shown that postoperative hemorrhage is 22.9% to 25% when using nasal packing and 3.12% to 4.65% when using a fibrin sealant. In fact, Vaiman and colleagues have shown that when using a fibrin sealant during septoplasties, their patients achieved complete resolution of major symptoms; good tissue approximation; and no hematomas, swelling, synechiae, atrophic changes, or adhesions. In contrast, in their group of patients in whom nasal packing was used, 36.5% of patients incurred some level of bleeding and additional discomfort, including sleep disturbance (93%), lacrimation (26%), and pain (47.2%).
Finally, it is important to be aware of unusual causes of bleeding from septoplasty. For example, if heavy intraoperative bleeding occurs, it could be secondary to rare occurrences, such as an internal carotid artery-cavernous sinus fistula causing a hyperemic and reactive nose. Be aware of additional signs and symptoms of this complication, including a developing orbital proptosis, deterioration of visual acuity, and pulsating tinnitus.
Cerebrospinal Fluid Leak: Early
Another complication of septoplasty that is exceedingly rare but deserves discussion is CSF leak. This complication is caused by a tear of the dura mater surrounding the brain and its supporting structures of the skull base, which therefore produces a leak of fluid through the formed connection between the subarachnoid space and the nasal cavity. This problem is extremely unusual after septoplasty, but it can be a serious and life-threatening complication if not managed quickly and appropriately. Nasal surgery is the second most common cause of CSF leakage, second only to traumatic skull base fractures. CSF leakage typically occurs early on in the postoperative period, but it may sometimes be days before symptoms develop. Classic presentations include CSF rhinorrhea, headaches, and a salty or metallic postnasal drip.
The literature reports that CSF leakage can occur when elevating the septal mucoperichondrium with a Cottle elevator and tunneling too superiorly on the septum, beyond the limits of the ethmoid roof, or by fracturing the perpendicular lamina, which subsequently can fracture the cribriform plate. These areas are at risk because of an intimate connection of dura to a weak and thin bone structure. The anterior cranial fossa is the usual site of this complication, with the roof of the ethmoid sinus and the cribriform plate as the most common sites. CSF leaks in the roof of the frontal and sphenoid sinuses are more likely to occur during endoscopic sinus surgery rather than during septoplasty surgery. When performing a septoplasty and a high bony septal deviation needs to be addressed, a controlled break of the perpendicular plate with a 4-mm chisel or Caplan scissors provides safe separation of the perpendicular plate from the skull base ( Fig. 2 ). This is particularly important to remember when repairing a nasal septal fracture, especially in the case of a “twisted” nasal septum when the dorsal septum is already malpositioned, likely requiring manipulation.
Early recognition of this complication is important. CSF rhinorrhea may be the first sign. In some cases, if a proper diagnosis is not made, there can be enlargement and remodeling of the bone over time and a dural defect, leading to herniation of the meninges and brain tissue through the defect by pulsation of the brain. This type of skull base defect after septoplasty would subsequently put the patient at risk for an ascending infection. The patients can sometimes present late with the symptoms of meningitis. If septoplasty surgery is performed extremely superiorly in the nasal cavity, avoidance of barometric pressure changes is recommended for 4 weeks after surgery.
The best way to minimize CSF leakage complications after septoplasty is through prevention and early diagnosis. Tawadros and Prahlow have shown that the risk for having a CSF leak after nasal surgery is increased in patients with a low-lying cribriform plate of the ethmoid roof, specifically found at a level inferior to two thirds of the orbit height on the preoperative CT scan. It is also imperative to prevent this complication with good realization and preoperative awareness of anatomic variations and a less aggressive septoplasty method, especially when manipulating the perpendicular plate attached to the ethmoid roof.
If CSF leak has occurred, antibiotics should be given immediately for meningitis prophylaxis. Conservative management of CSF leaks is preferred, with placement of a lumbar drain, reserving surgical repair for patients with a persistent leak despite these therapies. The defect may be approached endoscopically or transcranially to allow for a multilayer repair. If this complication occurs during surgery, it can be repaired endoscopically at that time once informed consent for the additional procedure is obtained. Preoperative informed consent for the septoplasty should include this information, but stopping to inform the patient’s family and obtain neurosurgical consultation is recommended. Surgical treatment options for CSF leak repairs include intra- and extracranial approaches, in addition to transcranial approaches, if you need to prevent recurrent meningitis in patients with large defects. Transnasal endoscopic repair is now the standard technique being performed. It is critical to note that meningitis and hydrocephalus can impair the endoscopic correction of a CSF leak and may lead to a poorer surgical outcome.
Infection: Early-Intermediate
As with any surgical procedure, postoperative infection is an important complication to prevent. Overall, there is a 0.48% to 2.5% chance of infection occurring secondary to septoplasty surgery, with infection most likely to occur immediately after surgery. Postoperative septoplasty infections are typically localized to the septum and nasal cavity, but they can rarely occur in the form of more dangerous threats, such as meningitis, cerebritis, subdural empyema, brain abscess, and even cavernous sinus thrombosis.
The pathogenesis behind infections after septoplasties stems from the fact that the upper respiratory tract is colonized with many normal bacterial floras. The mucous membranes act as a protective barrier and aid in processing foreign bodies. During septoplasty, those mucous membranes are traumatized and can put the patient at risk for infection and bacteremia by the vascular route within the nasal mucous membranes. There is evidence of transient bacteremia that occurs during open septorhinoplasty. Transient bacteremia is usually harmless in healthy subjects and usually resolves spontaneously without complications; however, the possibility of bacteremia during septoplasty surgery must be kept in mind, and the necessary precautions should be taken before surgery in patients with high risk for cardiovascular infection because this can lead to a dramatic result. Additionally, if septoplasty involves the use of nasal packing for 48 hours after surgery, the risk for bacteremia increases. Even when there is no bony laceration, intracranial infection can occur by direct invasion by way of venous and lymphatic channels of the mucoperiosteal lining of the nasal septum, which is frequently traumatized during septoplasty.
Some patients undergoing septoplasty may be predisposed to infection. It is known that nasal septal deviation impairs mucociliary transport. Septoplasty surgery to fix a deviated septum can significantly improve mucociliary transport; however, the procedure does impair mucociliary transport in the intermediate postoperative stages. Complete recovery of this transport system is established 5 days after surgery if the basal cells and basement membrane of the mucosa remain intact. As noted here, the change in the mucociliary transport system might contribute to an altered nasal mucosal pathogen environment after surgery. Eviatar and colleagues have found that although there is not a major difference in bacterial cultures before and after surgery, as implied by the dominance of Staphylococcus aureus , a change in nasal culture results does exist. So, although surgery does not completely disrupt the balance among nasal bacteria, changes in the cultures in the first postoperative month might indicate that the procedure caused mucosal abnormalities secondary to secretions, stasis, crusting, and packing after surgery. These events and circumstances suggest the importance of local environmental factors, aside from growth of bacteria in blood-absorbent packing matrix, in promoting the growth of S aureus .
Although transient bacteremia may occur and be completely asymptomatic, there have been reported cases in which the dangerous systemic toxic shock syndrome has occurred secondary to septoplasty. S aureus , considered an important pathogen in the genesis of nosocomial infections, is a frequent cause of bacteremia in postoperative patients. Most physicians credit the nasal packing as the mechanism behind this severe infection. The mechanism is compared with toxic shock syndrome secondary to tampon use on a large mucosal surface. When systemic changes, such as fever, diffuse erythroderma and subsequent peripheral desquamation of the hands, hypotension, vomiting, diarrhea, and multisystem complaints with laboratory abnormalities, take place, the patient should be treated promptly, with removal and culture of the nasal packing and hospitalization for the administration of fluids, empiric antistaphylococcal antibiotics, and possibly vasopressor medications. This condition warrants early suspicion, recognition, and initiation of appropriate treatment so as to avert significant morbidity and mortality. Given this potential risk and patient discomfort, it may be beneficial to avoid nasal packing unless it is required for uncontrolled bleeding, which is rare.
Septoplasties are considered potentially contaminated operations, but the proportion of patients developing a postoperative infection is small; therefore, perioperative systemic or postoperative antimicrobial prophylaxis is unnecessary. Caniello and colleagues have found that regardless of whether or not antibiotics are used, there is no concerning difference in terms of pain, fever, nausea, vomiting, bleeding, and purulent secretions. In addition, the downside to the indiscriminant use of antibiotics includes severe complications, such as toxic reactions and reduction of the antibody formation stimuli, in addition to representing high costs and encouraging less strict compliance with good surgical practice. The senior author (SAG) regularly provides preoperative antibiotic prophylaxis before induction for all patients undergoing septoplasty. Postoperative antibiotics are given only to those patients who have structural grafting or some type of splint or packing placed. In this situation, 3 to 5 days of treatment should be sufficient.
Again, as with any surgical procedure, there are some circumstances in which antibiotics are necessary. Patients with significant comorbid immune-related conditions, such as diabetes or compromised immunity, may receive prophylactic antibiotics. After surgery, in cases of acute or chronic infection of the operative site, use of cartilage grafts, implantation of allogenic materials, presence of a hematoma, mechanical blockage attributable to nasal packing, or postoperative nasal obstruction producing rhinosinusitis, antibiotics should be administered.
Septal Hematoma or Abscess: Intermediate
If unrecognized and not treated, septal hematoma is a significant complication of septoplasty. A septal hematoma may arise in the dead space created between the mucoperichondrial flaps when the cartilage or bony septum is removed during septoplasty. This space is susceptible to accumulation of blood products and the formation of a septal hematoma. The hematoma that forms after surgery can itself lead to several other complications, including ischemia and necrosis of the septal cartilage, decreased septal support, and impaired nasal function. A septal hematoma may also subsequently lead to the formation of a septal abscess, with Staphylococcus , Haemophilus influenza , and, rarely, Pseudomonas being the most common pathogens ( Fig. 3 ).



