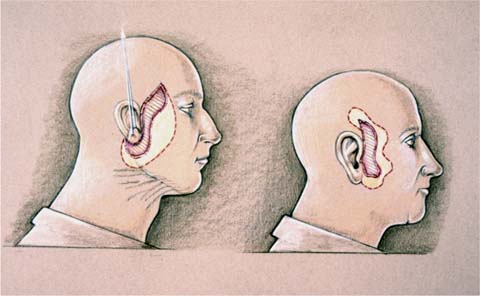
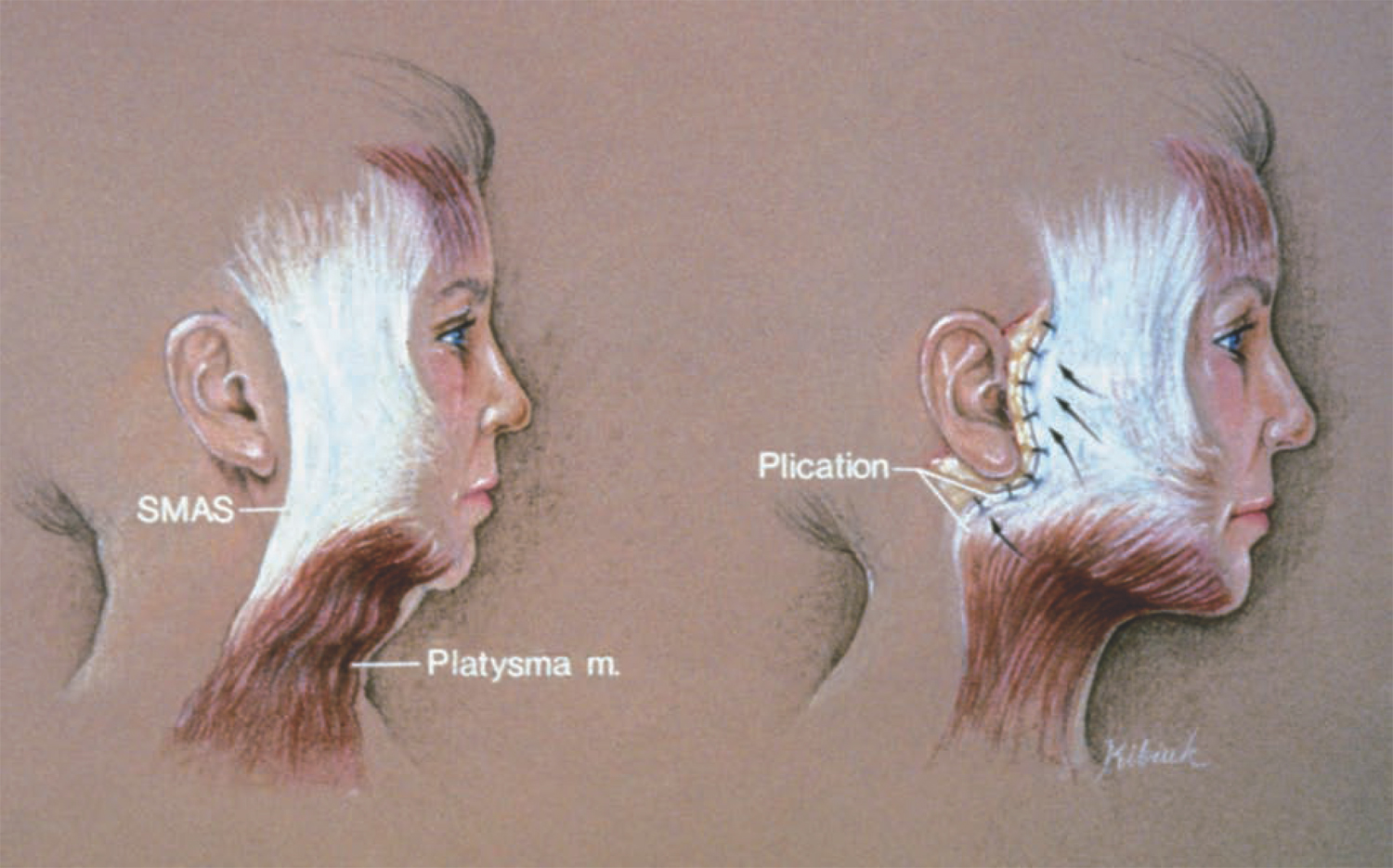
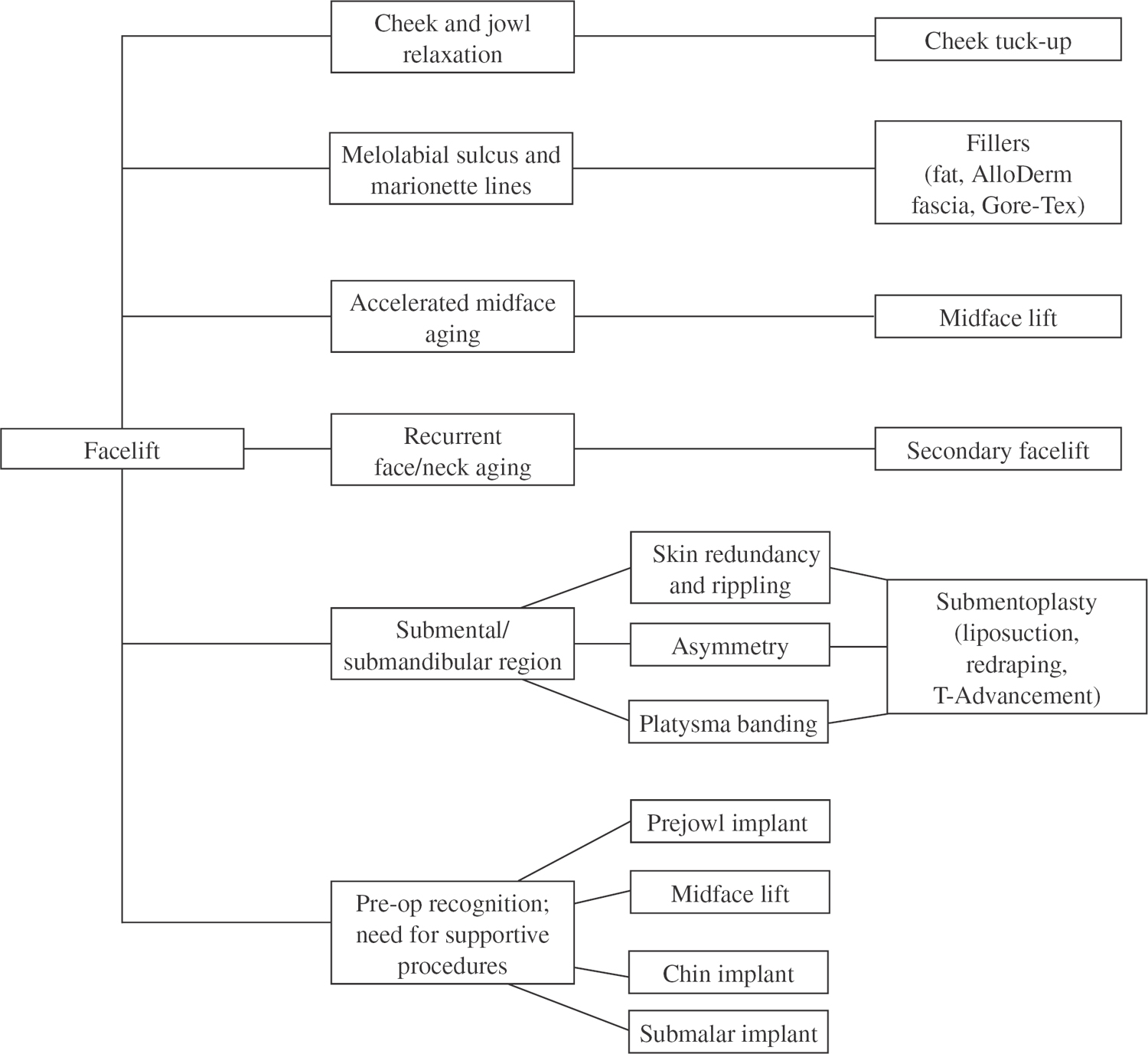
34 Secondary Rhytidectomy Rhytidectomy, or facelift, has been part of plastic surgery for over a century. And for probably just as long, patients have been unhappy with the results; hence the need for secondary procedures. We begin this chapter with an overview of the history of surgical techniques, focusing on the conflict in perceptions between surgeons and patients. We look at patient expectations and facelift limitations as well as patient selection as a predictor of revision facelift. Next, we review the types of revision surgery, particularly submentoplasty and cheek-only tuck-up facelift, and end with a discussion of new techniques that can reduce the incidence of revision or tuck-up procedures. Trying to enhance one’s appearance by “turning back the clock” surgically has been a pursuit of individuals for at least the past century. Cosmetic surgeons began to develop rejuvenation surgery procedures, particularly facelift surgery, in the early 1900s. Some of the early efforts were pioneered by German and French surgeons. In 1906, Lexer was thought to have performed surgery to treat wrinkles, but it was Hollander in 1912 who was the first to report a surgical case. Other European physicians, including Joseph (1921) and Passot (1919), developed their own techniques to treat the sagging, aging face.1 Early facelifting techniques consisted of very limited subcutaneous dissections, with skin elevation and tightening relying solely on the skin layer itself (Fig. 34.1). Unfortunately, this often resulted in a very temporary improvement, and occasionally an overzealous tightening of the skin resulted in an obvious operated look. Samuel Fomon, who was a pioneer in facial cosmetic surgery, recognized the limits of this type of facelifting procedure and of facelifts in general. According to Fomon, “The average duration of the beneficial effects, even with the best technical skill, cannot be expected to exceed 3 or 4 years.”2 Many of the early surgical techniques were not well publicized or talked about by plastic surgeons, as there was a prevailing attitude against vanity surgery. However, beginning in the late 1950s, and certainly by the early 1970s, there was a significant effort made to develop a surgical procedure that would offer long-lasting results yet leave the patient with a cosmetically pleasing, natural look. From a surgeon’s perspective, the ultimate facelift would be one that was predictable, had a low instance of complications, was technically feasible, and could be performed in a relatively short, efficient period of time. From a patient’s perspective, the surgical technique would be minimally invasive yet effective and last as long as possible, leaving the individual with a natural appearance. This difference between a more invasive procedure that created a fundamentally altered appearance but offered long-lasting results and a shorter, less invasive operation that improved the patient’s appearance with minimum recovery time but with short-term results emphasized the conflict in perceptions between the surgeon and patient as well as misconceptions about what can be expected from a facelift. It is interesting to note that the original facelifts performed were skin lifts only. Some of the most recent literature describing such “S-lifts” seem to advocate a return to these same early procedures that were found to be of limited benefit over a long period of time.3 Often “new” techniques such as S-lifts, or mini-facelifts, attract patients because they are minimally invasive, require only a short period of recuperation, and are reasonably low cost. However, they rarely satisfy the expectations of the patient or the surgeon. From a surgeon’s perspective, the pursuit of the ideal facelift procedure has created a great deal of different opinions and philosophies as to how to achieve natural, long-lasting results and a satisfied patient population. Much of this problem is due to the inherent limitations of the facelift procedure, no matter which technique is employed. It is an expensive operation, is technically involved, requires significant recovery time for the patient, and is inherently flawed. Both the patient and the surgeon are less than completely satisfied no matter how good the results may be for the given individual. Early discussions in the literature compared short skin flap elevations with long complete flap elevations. Cosmetic surgeons such as Richard Webster realized and demonstrated that lifting the underlying fascia and muscular layer often gave a nice improvement in the jaw- and neckline with fewer skin complications and a more natural appearance.4 This fascial layer was anatomically described by Mitz and Peyronnie in 1976 as the superficial muscular aponeurotic system (SMAS) (Fig. 34.2).5 Webster performed a comparison of plication (folding over and suture suspension) of this layer with relatively short skin flap elevation to large skin elevation with skin lifting only. Surgeons such as Skoog realized the benefits of the subfascial plane dissection as well and performed large elevations below the SMAS layer, treating the movement of the SMAS and the overall skin subcutaneous tissue as a sliding tectonic plate.6 This imbrication (advancement, shortening, and suturing) technique became the mainstay of facelift surgery and has been recently repopularized through the extended SMAS and deep plane techniques. Decision tree for secondary rhytidectomy Fig. 34.1 Passot’s 1910 “skin only” lift with limited or no undermining. Fig. 34.2 Plication of superficial muscular aponeurotic system (SMAS). Over time, surgeons were observing in their patients not only recurrent sagging of the skin and SMAS tissues but also significant recurrent banding of the platysma muscle in the neck (Fig. 34.3). Techniques not only to correct the platysmal banding but also to prevent it from recurring were developed, including anterior plication techniques, various anterior border muscular myectomy techniques, and direct transection of each playtsma muscle from side to side.7 Each of these techniques, however, fails to prevent recurrent platysmal banding in some patients and can create ridges of platysma or submental “cobralike” appearances. In recent years, with the development of the extended SMAS rhytidectomy,1 the biplane and triplane rhytidectomy of Baker,8 the deep plane techniques of Kamer,9 the composite rhytidectomies by Hamra,10 and the subperiosteal dissections by Ramirez,11 more aggressive surgical interventions were driven by the desire of surgeons to achieve a fundamental improvement that could be counted on to last for a significant length of time. As these techniques became more aggressive, increased levels of complications by relatively less experienced surgeons began occurring. In addition, the greater the degree of surgical intervention, the longer the healing phase or recuperation time for the patient. Patients became disenchanted with 6 weeks to 6 months of healing to achieve a “natural appearance” from their facelift. Increased competition among surgeons for facelift patients has brought the entire range of surgical techniques full circle. Some surgeons today are advocating “neck only” facelifts, midfacelifts, “laser” facelifts, and even endoscopic facelifting with essentially no skin redraping. There are increasing marketing claims of facelifts that allow the patient to fully recover and return to work over a weekend. Each of these procedures has significant limitations and significant incidences of recurrence of sagging with return of the aging face appearance, creating a dissatisfied patient population. Fig. 34.3 (A) Preoperative platysmal banding and (B) postoperative recurrent platysmal banding. Each patient asks his or her potential surgeon this fundamental question: How long is my facelift result going to last? It is generally expected that a given facelift procedure should last for at least 8 to 10 years. However, there are significant variations from patient to patient and preexisting condition to preexisting condition that can affect this average. There are certainly cases that one would expect to have significant recurrence of laxity and platysmal banding based on the preexisting condition, and these recurrences may be visible to the patient within the first 1 to 2 years. This creates relative dissatisfaction in an otherwise happy patient. There are also certain patients on whom a facelift result may last 12 to 15 years or longer in terms of a rejuvenated jawline and neckline compared with the preoperative condition. This mostly has to do with the preexisting elasticity, or lack thereof, and the patient’s individual hereditary tendency. Photoaging and smoking, for example, will at least accelerate, or even partially cause, a premature loss of elasticity, increased wrinkling, and early relapse of the prefacelift conditions with a significant diminution of the aesthetic result. Still, patients can be told that, following a facelift, they will continue to look younger, by 5 to 10 years, even though they will continue to age in a normal fashion because of their hereditary tendency, preexisting conditions, and lifestyle choices. Fundamentally, each patient, and, for that matter, each surgeon, desires a long-lasting improved jawline with minimum jowling, a well-contoured neckline with minimum to no platysma banding, and a naturalness to the overall look with relatively smooth skin. Therefore, secondary or tuck-up facelift procedures are required and are necessary to improve and maintain the primary facelift results. One of the more common areas of patient misunderstanding as to what facelifts will and will not do is the cheek–lip groove and fold, or the melolabial groove and fold. A standard cheek–neck facelift has very little effect on the upper third to upper half of this fold. There are techniques involved in midfacelifting, with particular attention to repositioning the middle cheek fat pad, that have some effect on this groove. Unless these are added to the operative procedure, patients need to understand that this is an area where very little improvement will be noted at the 6-month to 1-year postfacelift mark (Fig. 34.4). Another area of concern is the downward turn to the corner of the mouth. This oral commissure groove, which can extend to a significant “marionette line,” is only partially corrected with standard facelifting techniques (Fig. 34.5). By lifting the jowl and soft tissues of the lower third of the cheek, the marionette line is significantly effaced. However, the oral commissure itself is not affected by standard facelifting techniques (Fig. 34.6). Recurrence or persistence of this can be an area of dissatisfaction for the patient. Wrinkles or rhytides that exist within the surface of the skin may look better, if not significantly better, with facelifting. However, when the edema resolves and the tissue rebound relaxation occurs, most of these rhytides will still be present, and the patient needs to be educated about this fact in the preoperative consultation. None of these issues relate to a need for secondary or revision facelift surgery. They are just related to the limits of the procedure itself, and the patient’s expectations must be in concert with this prior to surgery. Fig. 34.4 (A)
Improving or Maintaining the Primary Facelift Results: Conflicting Perceptions

Patient Expectations and Facelift Limitations

![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


