Purpose
To investigate recruitment rates of patients with central retinal vein occlusion (CRVO) into phase III clinical trials evaluating intravitreal pharmacotherapy for treatment of macular edema in the United States, describe recruitment techniques in the Study of COmparative Treatments for REtinal Vein Occlusion 2 (SCORE2), and assess which SCORE2 recruitment techniques were most useful to principal investigators and clinical coordinators.
Design
Retrospective survey within a randomized clinical trial.
Methods
Recruitment rates of the Standard Care versus COrticosteroid for REtinal Vein Occlusion (SCORE)-CRVO trial, CRUISE Study, and SCORE2 were calculated. Techniques employed to facilitate recruitment in SCORE2 are described, and a survey was sent to the principal investigator and primary clinical coordinator of each SCORE2 site to assess the usefulness of recruitment techniques.
Results
In SCORE2, the recruitment rate of 0.39 participants/month/site was higher than in SCORE-CRVO (0.10 participants/month/site) and CRUISE (0.23 participants/month/site). For study design factors in SCORE2, investigators and coordinators rated provision of standard-of-care treatments to all study participants as having a major positive impact on recruitment. A monthly e-newsletter to site staff and communication by physician members of the SCORE2 Executive Committee to sites upon each randomization were perceived as effective means to help site staff focus on recruitment.
Conclusions
The SCORE2 recruitment rate compares favorably to previous clinical trials investigating intravitreal pharmacotherapy for treatment of CRVO-associated macular edema. Study design factors, methods of communication with sites, and recruitment techniques implemented in SCORE2 were well received by investigators and coordinators and may be helpful in future clinical trials.
Timely recruitment of a sufficient number of study participants to achieve the target sample size represents one of the most challenging aspects of a clinical trial. The American clinical pharmacologist Louis Lasagna observed that, when a clinical trial commences, the supply of suitable patients becomes a fraction of what it was assumed to be prior to the commencement of the trial. Lasagna’s Law refers to the observation that the number of patients available for entering a clinical trial falls markedly at study initiation and rises markedly after study completion. Muench’s Third Law states that, in order to be realistic, the number of cases promised in any clinical study must be divided by a factor of at least 10. Potential reasons for overestimation of patient availability for clinical trials may include such factors as restrictive clinical trial eligibility criteria, high refusal rates among eligible patients, and insufficient or ineffective resources to approach eligible patients.
Slow recruitment into the Standard Care versus COrticosteroid for REtinal Vein Occlusion (SCORE)-CRVO trial prompted a downward revision of the target sample size, and prompted the trial’s leadership to implement several techniques designed to optimize patient recruitment into the Study of COmparative Treatments for REtinal Vein Occlusion 2 (SCORE2). The current study was designed to investigate recruitment rates of patients with central retinal vein occlusion (CRVO) into phase III clinical trials investigating intravitreal pharmacotherapy for treatment of macular edema in the United States (US), to describe methods of communication with sites and recruitment techniques in SCORE2, and to investigate which of these activities were most useful to SCORE2 site principal investigators and clinical coordinators.
Methods
SCORE2 is a multicenter, prospective, randomized clinical trial designed to determine if bevacizumab is noninferior to aflibercept for the treatment of decreased vision due to macular edema associated with CRVO. The SCORE2 protocol and informed consent were approved prior to participant enrollment by the respective clinical center’s institutional review board (IRB) or a centralized IRB (Chesapeake IRB, Columbia, MD).
Study participant recruitment rates of all phase III clinical trials investigating intravitreal pharmacotherapy for the treatment of decreased vision due to macular edema associated with CRVO and conducted solely at clinical sites in the US were calculated based on information provided in the publications of these studies (total number of study participants recruited, dates of enrollment, number of clinical sites). Clinical trials included in the current study are the SCORE-CRVO, CRUISE and SCORE2 trials. The GENEVA Study is not included because it was not conducted solely at sites in the US (it was conducted at 167 sites in 24 countries throughout the world) and it included patients with CRVO and patients with branch retinal vein occlusion (BRVO). The COPERNICUS and GALILEO trials are not included because they were not conducted solely at sites in the US (the GALILEO trial was conducted across 63 sites in Europe and the Asian-Pacific region and the COPERNICUS trial was conducted at 70 sites in the US, Canada, India, Israel, Argentina, and Colombia).
An on-line survey of communication methods and recruitment techniques was constructed and e-mailed to the SCORE2 principal investigator and primary clinical coordinator at each of the 75 SCORE2 clinical sites that completed study requirements to participate in recruitment, including sites that did not randomize any SCORE2 participants. One SCORE2 clinical site had withdrawn early in the recruitment period and, therefore, was not administered the survey. Response to the site survey on recruitment techniques was good, with 69 of the 75 sites (92%) submitting at least 1 survey, for a total of 99 surveys submitted. The survey was completed by 65 of 75 (87%) primary clinic coordinators and 34 of 75 (45%) principal investigators. The survey asked questions about the perceived impact of specific study design factors on the site’s ability to recruit using a 5-point Likert scale: “1-Major hindrance,” “2-Minor hindrance,” “3-No impact,” “4-Minor positive impact,” and “5-Major positive impact.” The survey also focused on recruitment tools and communication methods to aid recruitment, and within each of these domains, the questions fell into natural pairs: (1) utility of the tool or communication based on whether or not it was used or site staff recalled receiving; and (2) perceived helpfulness of the tool or communication with responses on a 5-point Likert scale covering “Not at all,” “Slightly,” “Moderately,” “Considerably,” and “Extremely.” For analysis, both members of the pair of questions were combined together, so that responses follow a rank order from “Did not use it” to “Used it, and extremely helpful.”
Mostly descriptive analyses are presented, with t tests and χ 2 tests for some comparisons. All analyses and interpretations should be viewed as exploratory in nature.
SCORE2 is registered on http://www.clinicaltrials.gov (identifier: NCT01969708 ).
Results
In SCORE-CRVO, 271 patients were enrolled from 66 clinical sites over 40 months, between November 2004 and February 2008, for an average recruitment rate of 6.7 patients per month (0.10 participants/month/site). In CRUISE, 392 patients were recruited from 95 clinical centers over 18 months, between July 2007 and December 2008, for an average recruitment rate of 21.7 patients per month (0.23 participants/month/site). In SCORE2, 360 patients were enrolled from 66 clinical sites over 14 months, between September 2014 and November 2015, for an average recruitment rate of 25.7 patients per month (0.39 participants/month/site).
Communication methods and recruitment techniques employed in SCORE2 were aimed at study investigators, coordinators, and potential participants to help meet enrollment goals. Engagement of investigators through conference calls and webinars took place during trial planning, soliciting feedback on trial design that focused not only on the scientific aspects of the study but also on operational characteristics that would facilitate recruitment. Four study design features were included in the survey for feedback from the site principal investigator and clinical coordinator as to the impact of that particular trial design feature on the site’s ability to recruit, as displayed in the Table . All 4 of the study design features were felt by principal investigators and clinical coordinators to be important based on mean scores between 4 (minor positive impact) and 5 (major positive impact). In particular, both the site principal investigators and the coordinators perceived that all study participants receiving standard-of-care treatments, with absence of an untreated control arm, was positively impactful for recruitment, with 85% of principal investigators and 79% of coordinators noting this factor as having a major positive impact on recruitment.
| Principal Investigator (N = 34) | Clinical Coordinator (N = 65) | |||
|---|---|---|---|---|
| Mean Score | % Noting Major Positive Impact | Mean Score | % Noting Major Positive Impact | |
| Eligibility criteria allowed for prior use of anti-VEGF treatment | 4.15 | 50.0% | 3.89 | 35.4% |
| SCORE2 supply of study drug | 4.53 | 70.6% | 4.68 | 78.5% |
| All study participants received standard-of-care treatments and there was no untreated control arm (eg, sham injection, observation) | 4.76 | 85.3% | 4.62 | 78.5% |
| Ability to screen and randomize on 1 day | 4.53 | 67.7% | 4.43 | 61.5% |
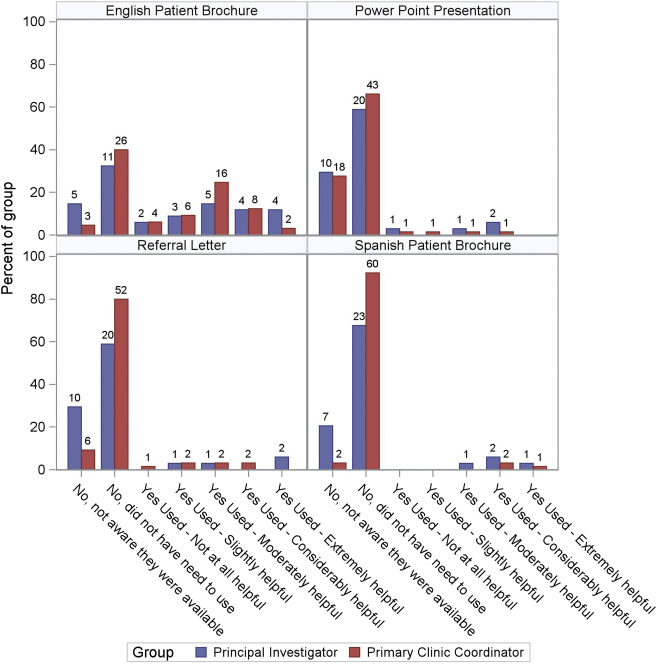
A number of recruitment aids were made accessible to site staff at the outset of SCORE2 on the study website, including a patient brochure in English and Spanish to help patients better understand SCORE2, a SCORE2 PowerPoint presentation to allow investigators to lecture locally about SCORE2 and thus increase eligible referrals to their clinical site, and a physician referral letter template made available to clinical site investigators to allow them to send letters to local eye care providers to refer potential eligible patients. Figure 1 shows the responses from the principal investigators and primary clinical coordinators; in general, the PowerPoint presentation, referral letter, and Spanish patient brochure were not used. The English patient brochure was noted to be used approximately 50% of the time, with 13 principal investigators (38%) and 26 clinical coordinators (40%) rating it moderately, considerably, or extremely helpful.
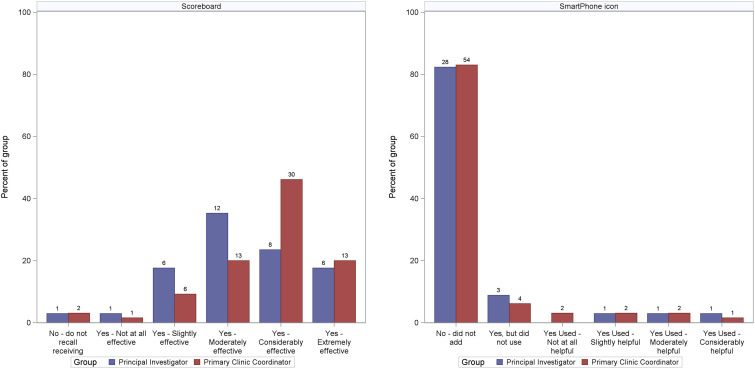
Communication by the Executive Committee (EC) and the Data Coordinating Center (DCC) was another major focus during recruitment. These included the SCOREBOARD, a monthly e-newsletter designed to keep SCORE2 site staff informed about study progress and provide information about upcoming timelines and events; and a SCORE2 icon for Apple and Android smartphones, which provided site staff quick access to SCORE2 inclusion and exclusion criteria and the ability to communicate directly with an ophthalmologist on the SCORE2 EC and the DCC for both time-sensitive and non-time-sensitive issues. Figure 2 shows the responses, which note the mostly favorable ratings regarding the SCOREBOARD; this e-newsletter was recalled as being received and as being very useful, with 26 principal investigators (76%) and 56 clinical coordinators (86%) rating it moderately, considerably, or extremely helpful. The SCORE2 icon for Apple and Android smartphones was not widely taken advantage of in SCORE2, with 28 principal investigators (82%) and 54 clinical coordinators (83%) not using it.