Chapter 15
SCLERAL AND CORNEOSCLERAL INJURIES

Trauma is a common cause of corneoscleral and scleral defects in the young, otherwise healthy patient. Traumatic corneoscleral defects may take two forms:
1. those resulting acutely in the context of closed or open trauma; and
2. those occurring secondarily from tissue necrosis as a result of post-traumatic inflammation or infection.
Although the acute consequences can generally be repaired primarily, those occurring late often require repair by patching. When faced with the penetrating type of corneo/sclerala trauma, the clinician must rule out conclusively the presence of IOFBs and must evaluate and attend to intraocular damage.
Goals in the management of corneo/scleral injury include1:
• restoration of the integrity of the globe;
• avoidance of further injury to ocular tissues; and
• prevention of cornealb scarring and astigmatism.
Small, isolated scleral defects without uveal prolapse may respond to conservative management with observation and appropriate prophylactic antibiotic therapy. Larger wounds or areas of scleral thinning may require surgical repair, either by primary closure or by patch grafting.
PEARL… Successful surgical management of traumatic corneo/scleral defects requires identification of, and tailoring of the surgical approach to, the underlying mechanism of injury.
EPIDEMIOLOGY
The following information is from the USEIR database.
Incidence:
• rate of corneoscleral involvement among eyes with serious injuries: 10%;
• rate of purely scleral involvement among eyes with serious injuries: 30%.
Age (years):
• range: 0–101;
• mean: 32;
• ≤15: 22%;
• 20 to 39: 38%;
• ≥60: 11%.
Sex:
• males: 82%;
• among those aged 0 to 59 years, males outnumber females nearly 5 times;
• among those aged 60 to 69 years, males outnumber females 1.5 times;
• in the ≥70–year-old population, females outnumber males nearly 1.5 times.
Place:
• 44% home;
• 17% street and highway;
• 11% work.
Cause:
• 33% blunt object;
• 13% sharp object;
• 12% MVC;
• 12% fall.
Injury type (purely scleral, not corneoscleral injuries):
• rate of scleral ruptures among all scleral injuries: 28%;
• rate of scleral lacerations among all scleral injuries: 28%;
• rate of scleral ruptures among all ruptures: 54%;
• rate of scleral lacerations among all lacerations: 59%.
PEARL… Trauma inflicted by blunt objects plays a major role in corneo/scleral injury. The clinician must be alert for this type of injury in patients involved in MVCs and in falls (particularly among the elderly).
EVALUATION
History
A detailed history regarding the mechanism of injury directs the manner in which evaluation and repair will proceed. The clinician should address the following critical questions.
• Are there other life-threatening injuries that need to be addressed before repair of the ocular injury (see Chapters 9 and 10)?
• What was the exact mechanism of injury?
• If the injury resulted from an IOFB, what was the composition of the object, at what speed was it traveling, and what was the angle of impact to the eye/orbit (see Chapter 24)?
Surgical repair of corneo/scleral wounds may need to be delayed if other life-threatening injuries are present. Wound closure should take place, however, as soon as possible to avoid adverse sequelae such as infection. The mechanism of injury alerts the clinician to the possibility of occult scleral injuries, intraocular damage, and IOFBs.
Physical Examination
• Gentle separation of the eyelids may be required; avoid pressure on the globe (see Chapters 8, 9, and 14).
• Assess the visual acuity; and, using “naked” inspection and the slit lamp, assess (see Chapters 9, 12, and 14):
 periocular structures;
periocular structures;
 conjunctiva;
conjunctiva;
 cornea;
cornea;
 sclera;
sclera;
 pupil(s) and other anterior segment structures.
pupil(s) and other anterior segment structures.
• Ophthalmoscopy should also be attempted in the setting of obvious open globe injury and especially with uveal or vitreous prolapse. Dilating drops should not be used. In such cases, the remainder of the examination should be deferred to the more controlled operating room setting (see Chapter 8).
Preoperative findings associated with scleral rupture include2:
• visual acuity of light perception or NLP;
• chemosis;
• 360-degree subconjunctival hemorrhage;
• hyphema;
• IOP <10 mm Hg;
• peaked pupil (the apex of the peak is often aligned with the meridian of the rupture); and
• relative displacement of the lens-iris diaphragm (asymmetry of AC depths).
PITFALL
Scleral rupture may be occult and posterior. The clinician who pays attention to the (often subtle) signs of scleral rupture will not miss these injuries.
Careful preoperative examination of the patient with attention to the size and location of the corneo/scleral defect and the condition of the surrounding tissues allows the surgeon to plan the steps of exploration and repair. If a retinal tear/detachment or an IOFB is discovered preoperatively, involvement of a retinal surgeon in the primary repair is recommended.
Appropriate imaging studies of the orbits may have to be obtained preoperatively (see Chapter 9).
• Ultrasound is useful in the setting of small wounds where the risk of extrusion of intraocular contents is minimal.
• If CT scans are indicated, fine (<1.5 mm) cuts through the entire orbit, with axial and coronal images, are required so that small IOFBs will not be missed (see Chapter 24).
Other Issues
When a patient has concomitant systemic disease, the clinician must be alert to the possibility of an underlying inflammatory or infectious process that may predispose the patient to the formation of a scleral wound (see Chapter 20).
Inflammation: In a study3 of patients with autoimmune disease treated with scleral homografting for necrotizing scleritis, rapid graft melting occurred in those who did not receive chemotherapy before, or concomitant with, surgical intervention. The grafts remained stable, however, in those who received chemotherapy concomitant with surgery.c
Infection: Post-traumatic bacterial or fungal scleritis may cause scleral thinning and rupture/perforation. Surgery is often an important adjunct to antimicrobial therapy in these cases. Weakened sclera can be reinforced with a patch following débridement of devitalized tissue and harvest of material for culture. A readily vascularized patch provides optimal healing in this setting.
PITFALL
Lack of attention to, or treatment of, underlying infection or inflammation increases the risk of failure of the scleral repair.
Summary
The exact mechanism of scleral wound formation cannot always be determined preoperatively, particularly in acute cases or in patients with concomitant systemic disease. However, to achieve the optimal outcome for each patient, the surgeon should:
• establish the causative factors;
• institute medical therapy if indicated;
• carefully assess the extent of injury;
• exclude or confirm the presence of IOFBs; and
• plan a stepwise surgical approach.
see Chapter 27 for the strength of a healed wound.
ANESTHESIA
General Anesthesia
It is the preferred method for repair of corneo/scleral injuries because it:
• provides the dual benefit of excellent anesthesia and akinesia with minimal increase in intraocular/intraorbital pressure (see Chapter 8); and
• allows operative intervention at multiple sites for the harvest of fascia lata and other autologous graft material if and as necessary for the patching of large tissue defects.
General anesthesia may be inappropriate in patients who are:
• systemically ill;
• elderly; and/or
• debilitated.
Topical Anesthesia
It is suitable for small, anterior defects; but such defects are rare. Of all types of anesthesia available to the surgeon, the topical approach may carry the lowest risk of systemic stress and inadvertent injury to the globe. Topical anesthesia alone, however, is inadequate for the extensive dissection of conjunctiva and Tenon’s capsule required for repair of large or posteriorly located areas of scleral thinning or wound.
Retrobulbar Anesthesia
It provides excellent local anesthesia and akinesia with minimal cardiac and respiratory stress. However, injection of a retrobulbar anesthetic agent increases the intraorbital, and consequently the intraocular, pressure.
PITFALL
Retrobulbar anesthesia may put undue pressure on the traumatized globe, leading to prolapse of intraocular contents.
This anesthetic technique is most appropriate for the repair of defects too extensive for topical anesthesia or for patients in whom general anesthesia poses an unacceptable systemic risk (see Chapter 8).
TECHNIQUES OF OPERATIVE REPAIR
PEARL… A Jaffe-style lid speculum avoids undue pressure on traumatized tissues by lifting the palpebral circle off the globe via the force of the elastic bands.4
Tissue Adhesive
Tissue adhesived is:
• generally reserved for small, puncture-type wounds in which the overall integrity of the globe is not compromised; and
• useful in very small or partial-thickness corneo/ scleral lacerations.
Primary Closure
Scleral Wound
Figure 15–1 illustrates the technique of globe exploration and primary closure.
PEARL… Scleral ruptures most commonly involve weak or thin areas of the sclera such as at the limbus, just behind muscle insertions, and at the insertion of the optic nerve.
If an occult scleral wound is suspected, globe exploration is required.
• A 360° peritomy is made and Tenon’s capsule is retracted posteriorly to reveal the underlying sclera.
• The extraocular muscle insertions and the areas in between insertions are directly visualized. If necessary, a traction suturee may be carefully introduced under the muscle under meticulous direct observation.5
For wound closure, the following points have to be remembered.
• Scleral wounds are closed from anterior to posterior, beginning at a recognizable landmark such as the limbus or the apex of the laceration. Tight closure prevents fibrovascular proliferation through an open scleral wound.
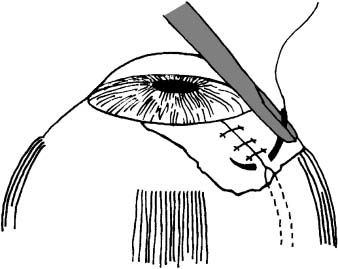
FIGURE 15–1 The “ close-as-you-go” technique for exploration and primary closure of a scleral wound. The conjunctiva and Tenon’s capsule are opened enough only to visualize the next suture site. In this manner, the periorbita maintains pressure on the scleral defect, thus keeping the intraocular contents stabilized until the lips of the scleral wound are apposed.
PEARL… If the scleral wound is large, the surgeon must close the visible/accessible portion before
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


