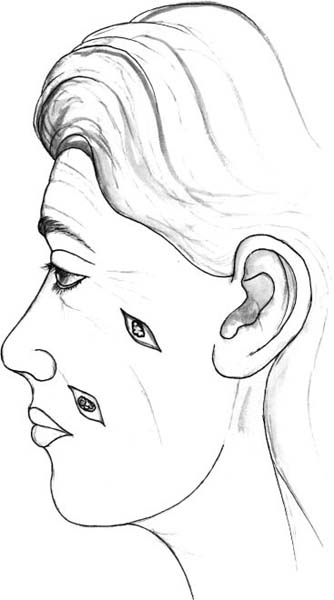
37 Scar Revision Surgery A wound that is allowed to heal under favorable conditions is most likely to produce an acceptable scar. The first documentation concerning scar formation is found in the Smith papyrus (1700 bc).1 The physicians of ancient Egypt, Greece, and India empirically appreciated the need to maintain clean wounds, minimizing wound irritation. Harsher methods such as hot cautery and boiling oil were later employed without scientific basis in Europe during the Middle Ages. The concepts of foreign body removal and sterility were largely ignored in favor of wound irritation and “laudable pus.” Obviously, such techniques resulted in slower healing and a disfiguring scar. Knowledge of wound healing has since been refined to minimize characteristics that might draw attention to a scar. The predictability of facial scarring depends partly on the etiology of injury. Causes of facial wounds include trauma, burns, elective procedures, and emergency surgery. Scars resulting from collisions or from tribal ceremonies will often contain varying amounts of debris and fibrosis. A well-planned sterile surgical incision is more likely to heal favorably than an avulsion injury sustained in a motor vehicle accident. Ideally, planned procedures should require lower rates of scar revision than traumatic injuries. However, improper tissue handling techniques, poorly designed incisions, and uneven wound edges can lead to unacceptable scars. Adverse wound-healing factors such as infection, excessive tension, presence of a foreign body, and prolonged presence of suture material may also contribute to the formation of obvious and unsightly scars. In certain situations, unappealing scars can develop despite a surgeon’s best efforts and optimal wound-healing conditions. Some individuals, particularly those of African, Hispanic, or Asian descent, are predisposed to keloid formation or hypertrophic scars. Information regarding a patient’s personal healing characteristics should be sought preoperatively. Wound healing is a dynamic process that undergoes numerous transformations before achieving a steady state. Prior to reaching its final appearance at approximately 1 year after tissue injury, a wound progresses through the phases of coagulation, inflammation, fibroplasia, and remodeling. The remodeling phase represents the stage of maturation during which intense fibroplasia, inflammation, and angiogenesis have subsided. Subsequently, a cycle of collagen deposition and lysis develops that continues in perpetuity. A scar will ultimately reach 80% of the tensile strength of normal skin.2 Scarring is a normal biologic reaction to tissue injury; no incision or cutaneous injury will heal without forming a scar. Therefore, the question regarding the nature of scarring after surgery does not pertain to if, but instead to what, extent. Failure on the part of the surgeon to adequately convey this fact may encourage the patient to foster unrealistic expectations. In scar revision surgery, the original scar should be carefully assessed for the amount of improvement that can be realistically obtained. The ideal scar should be flat, narrow, level with the surrounding skin, of good color match, within or parallel to relaxed skin tension lines, and sinuous.3 These properties make a scar less distinguishable from the expected skin contour, effectively camouflaging it. Obviously, there are limits to which a scar can be made less noticeable. With this in mind, attempts to further camouflage a scar that has met most of the above criteria are not advisable. There are many situations in which the patient and surgeon mutually agree that the appearance of a scar can be improved. Traditionally, an arbitrary waiting period of 6 to 12 months has been proposed prior to revision, allowing for scar maturation. However, appropriate early intervention is sometimes justified. Six to 9 weeks after tissue injury, a high degree of intrinsic fibroblastic activity exists. This serves as the basis for early dermabrasion of a wound.4 Certain scars show signs of functional compromise and/or unacceptable appearance at an early stage and will almost definitely require later revision. Precocious intervention is warranted in such situations. Examples include scars that are perpendicular to relaxed skin tension lines or facial anatomical landmarks such as the melolabial crease. The decision to revise a scar, the timing of this revision, and appropriate nonsurgical options should be discussed with the patient. If surgical intervention is decided upon, the manner in which it is accomplished depends on several factors: the position and orientation of the scar, its relationship to important anatomical sites, the thickness and quality of surrounding skin, and the size of the scar. A description of each technique and a critical analysis of its indications, benefits, and disadvantages are included below. The most important concept to be considered in excisional techniques is that of scar position. An ideally placed scar does not draw undue attention from surrounding facial features. Incisions should be placed within or parallel to relaxed skin tension lines (RSTLs), within lines separating facial anatomical subunits, or within the hairline to allow for appropriate camouflage. A basic principle of surgical therapy applies: the least complex form of therapy with acceptable results is frequently the best. A scar that lies within an RSTL or in a similar favorable position can be managed by fusiform excision (Fig. 37.1). Incisions that are perpendicular to RSTLs and those requiring opposing angles of > 60 degrees are not suitable for this technique. The superficial portion of the scar is excised in a fusiform shape, with opposing angles of 30 degrees or less. It is frequently helpful to leave the deeper component of the scar intact. This firm, mature scar tissue may augment the depth of the wound and help prevent a depressed surface to the scar. Excessively long incisions, those abutting important functional structures, or requiring angles between 30 and 60 degrees can be managed with an M-plasty. The M-plasty technique can prevent unnecessary removal of tissue or scar lengthening. Adequate undermining is often necessary to approximate wound edges in an even and tension-free manner. Subcutaneous and dermal closure is achieved using absorbable suture (usually 5–0 polygalactic acid suture), followed by cuticular closure with a monofilament suture (usually 6–0 polypropylene). The external monofilament sutures should be removed within 1 week. The cosmetic deformity caused by a scar can be simple or complex. A superficial irregularity can be tangentially shaved using a flexible razor blade or scalpel. Narrow scars with raised or uneven wound edges and small standing cutaneous deformities are suitable for this form of treatment. Shave excision can be done in conjunction with other scar revision techniques for portions of a scar. The excision should be superficial enough to level the scar with the surrounding skin, yet avoid entry into the deep dermis. After excision, the wound is allowed to heal by secondary intention. Fig. 37.1 The dynamic action of the facial musculature is responsible for the formation of relaxed skin tension lines (RSTLs). RSTLs are perpendicular to the underlying facial muscles. Placement of incisions should be within or parallel to RSTLs for optimal cosmesis in wound healing. The simplest form of scar revision involves excision of a scar in the form of an ellipse followed by primary wound closure. The appearance of a scar may be more noticeable or even objectionable due to its location. Some small scars lie close to RSTLs, important lines separating anatomical subunits, or the hairline and can be appropriately repositioned with excision of a small amount of intervening normal tissue. For example, selected scars can be repositioned into a nasolabial fold, preauricular crease, glabellar crease, or horizontal forehead rhytid.
Scar Analysis
Techniques in Scar Revision
Excisional Techniques
Fusiform Excision
Shave Excision
Scar Repositioning
Serial Partial Excision
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


