and Charles P. Molumi2
(1)
University of Papua New Guinea and Port Moresby General Hospital, Boroko, National Capital District, Papua New Guinea
(2)
Port Moresby General Hospital, Boroko, National Capital District, Papua New Guinea
4.1 Submandibular Sialoadenectomy

Fig. 4.1
The patient lies supine with the head slightly extended and tilted to the opposite side. The incisions lieds 2.5 cm below the mandible in the skin crease and curved upwards anteriorly
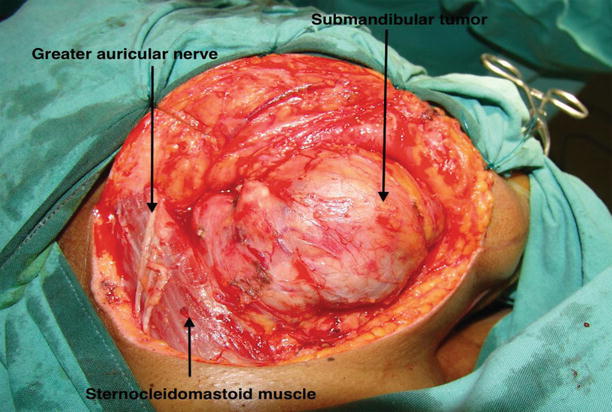
Fig. 4.2
Skin incision is carried below the platysma and subplatysmal flap raised exposing the submandibular gland with tumor. At the angle of the mandible, the facial artery and vein are identified, ligated and reflected upwards to protect the mandibular division of facial nerve. Elevation of the fascia over the submandibular gland further protects the nerve
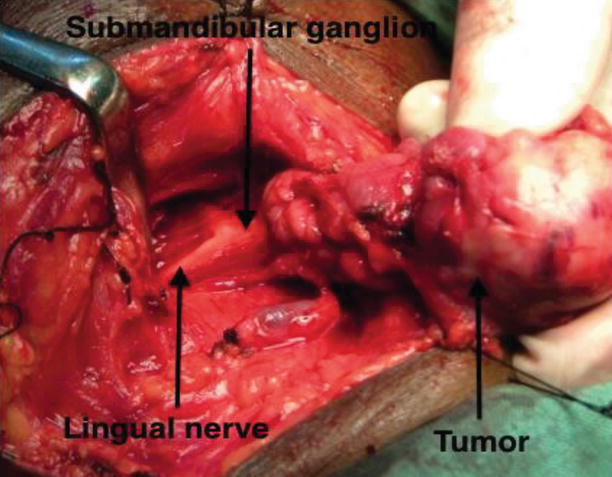
Fig. 4.3
The upper border of the gland is dissected from the mandible and anterior part of the gland in the submental region. The lower part of the gland is elevated by following the hyoid posteriorly to free the part of the gland which curves backwards over the mylohyoid muscle. The anterior part of the gland is held with a Allis forceps and the facial artery and vein entering the lower border of the gland are ligated. The posterior border of the mylohyoid muscle is retracted anteriorly exposing the submandibular duct which pull the lingual nerve into view in a ‘V’-Shaped curve
Fig. 4.4
The lingual nerve is dissected away from the gland and the submandibular duct is cut and ligated
Fig. 4.5
The submandibular gland is removed with the tumor. The specimen is examined in its entire form (a) and (b) cut section and sent for histopathological examination
4.2 Superficial Parotidectomy
Fig. 4.6
Modified Blair incision is marked out in the preauricular skin crease at the superior border of the helix and curried below the helix and below the lobule and then turned anteriorly to run horizontally in a skin crease approximately 2 fingerbreaths below the angle of the mandible
Fig. 4.7
The skin incision is carried to the subcutaneous tissue and platysma muscle. The greater auricular nerve as it runs over the sternocleidomastoid muscle is identified and preserved. The anterior flap is raised superficial to the greater auricular nerve and the parotid fascia. Elevation of the posterior and inferior flap exposed the tail of the parotid. The flaps are retracted with silk sutures. The tail of the parotid gland is dissected off the sternocleidomastoid muscle by dissection deep to the posterior branch of the greater auricular nerve
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


