Salivary Gland Surgery
Salivary gland excision may be required to remove a gland damaged by chronic infection or with a mass that may be a tumor.
29-1 Submandibular Gland Excision
Indications
Submandibular gland excision is indicated in the treatment of chronic salivary gland infections, salivary gland stones, suspicion of neoplasm, and as an adjunct to surgical treatment for drooling.
Preoperative Evaluation
Palpation of the submandibular gland is usually sufficient to detect a mass. Sialography defines chronic inflammatory disease, stones, or strictures. Computed tomography (CT) or magnetic resonance imaging (MRI) is a more appropriate study to evaluate masses in the submandibular area. Fine needle aspiration (FNA) may be helpful. The surgeon may elect to utilize intraoperative facial nerve monitoring.
Operative Technique
1. Submandibular gland excision is performed utilizing general endotracheal anesthesia.
2. The patient is positioned on a shoulder roll. The head is hyperextended and turned to the opposite side. This brings the submandibular gland into position (Fig. 29.1a).
3. One percent lidocaine with 1:100,000 epinephrine is injected in a skin crease near the lower border of the gland for hemostasis. This should be approximately 2 to 3 cm below the edge of the mandible to avoid the marginal mandibular branch of the facial nerve (Fig. 29.1b).
4. The platysma muscle is divided with a knife and minimal flaps are developed superiorly and inferiorly exposing the cervical fascia overlying the gland (Fig. 29.1c).
5. The cervical fascia is incised and the gland exposed (Fig. 29.1d). By staying deep to this fascia, injury to the marginal mandibular nerve, which lies between the platysma and the fascia of the gland, is avoided.
6. The facial artery and vein over the posterior aspect of the gland are divided (Fig. 29.1e) and elevated superiorly, further protecting the marginal mandibular nerve.
7. The submandibular gland is then mobilized by blunt and sharp dissection out of the digastric sling and off the hyoglossus muscle. The hypoglossal nerve deep to the gland is preserved and vessels are divided releasing the gland (Fig. 29.1f).
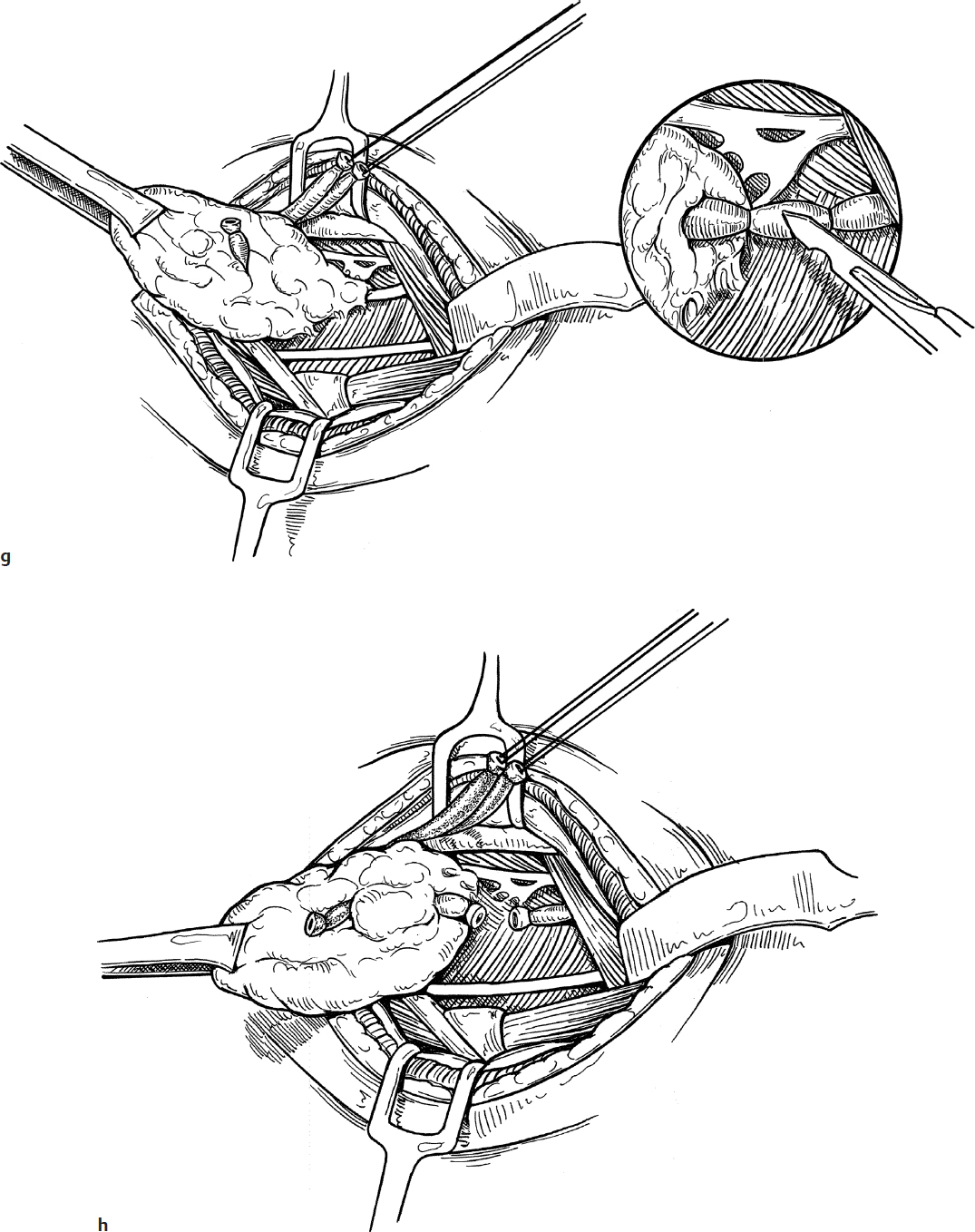
8. The mylohyoid muscle is then retracted anteriorly as the submandibular gland is retracted posteriorly (Fig. 29.1g). This stretches and exposes the duct, which should be double ligated with 3-0 silk and divided.
9. The gland is then retracted posterointeriorly and the submandibular ganglion and accompanying vein are transected with a knife, allowing the lingual nerve to retract up under the mandible and releasing the entire gland for removal (Fig. 29.1h).
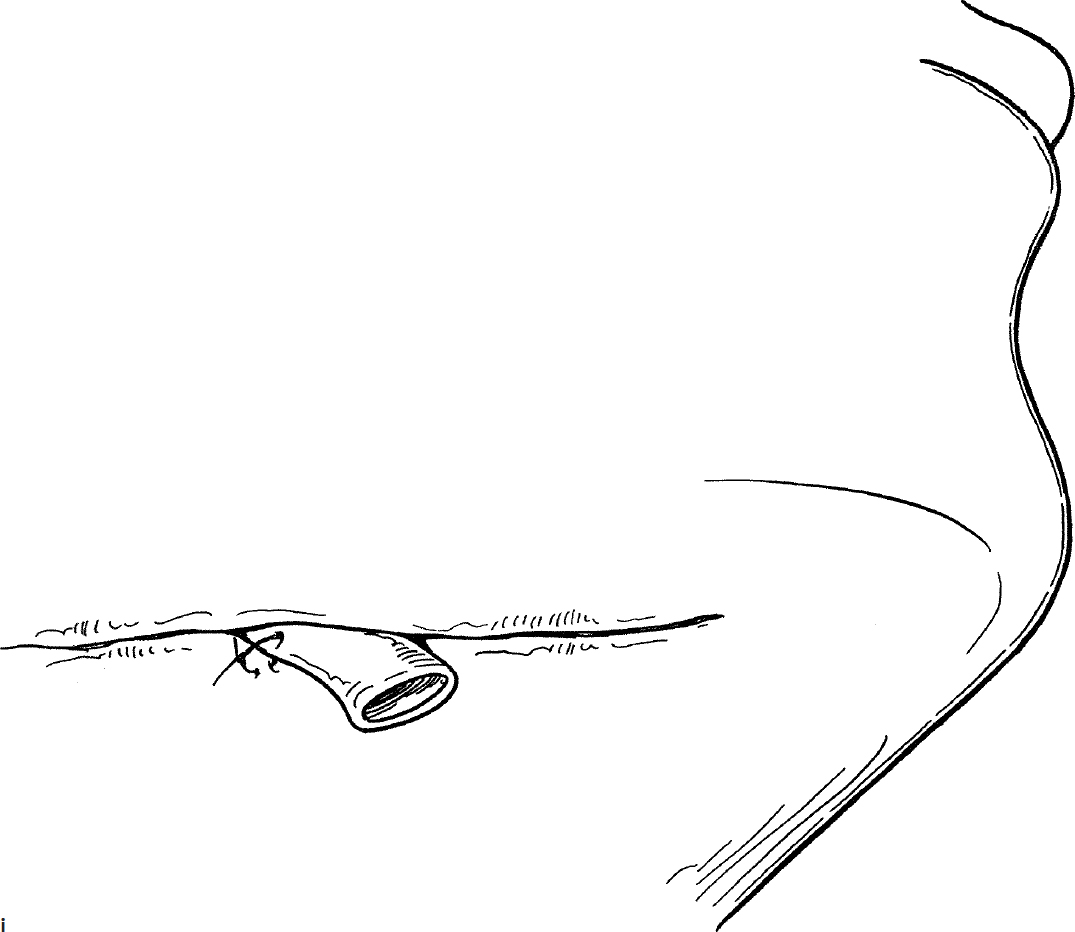
10. The wound is closed in layers (platysma, subcutaneous tissue, and subcuticular chromic) and a small Penrose drain is placed in the wound (Fig. 29.1i). The drain is removed in 12 to 24 hours.
Complications
1. Marginal mandibular nerve injury
2. Hypoglossal nerve injury
29-2 Parotidectomy
Introduction
Parotidectomy is most commonly performed in children to excise a mass (suspected neoplasm) in the parotid gland. Rarely, parotidectomy may be required to treat chronic inflammatory disease or stones.
Indications
A mass in the parotid gland and chronic and recurrent parotitis are indications for parotidectomy.
Preoperative Evaluation
Sialography, CT, or MRI may help define a mass in the parotid gland, but these studies do not have histologic specificity. An FNA may be appropriate in a cooperative patient. A suspected neoplasm must be removed for treatment and histologic diagnosis. The surgeon may elect to utilize intraoperative facial nerve monitoring.
Operative Technique
1. Parotidectomy is performed utilizing general endotracheal anesthesia without the use of any long-acting paralyzing agents. This permits intraoperative facial nerve monitoring and stimulation.
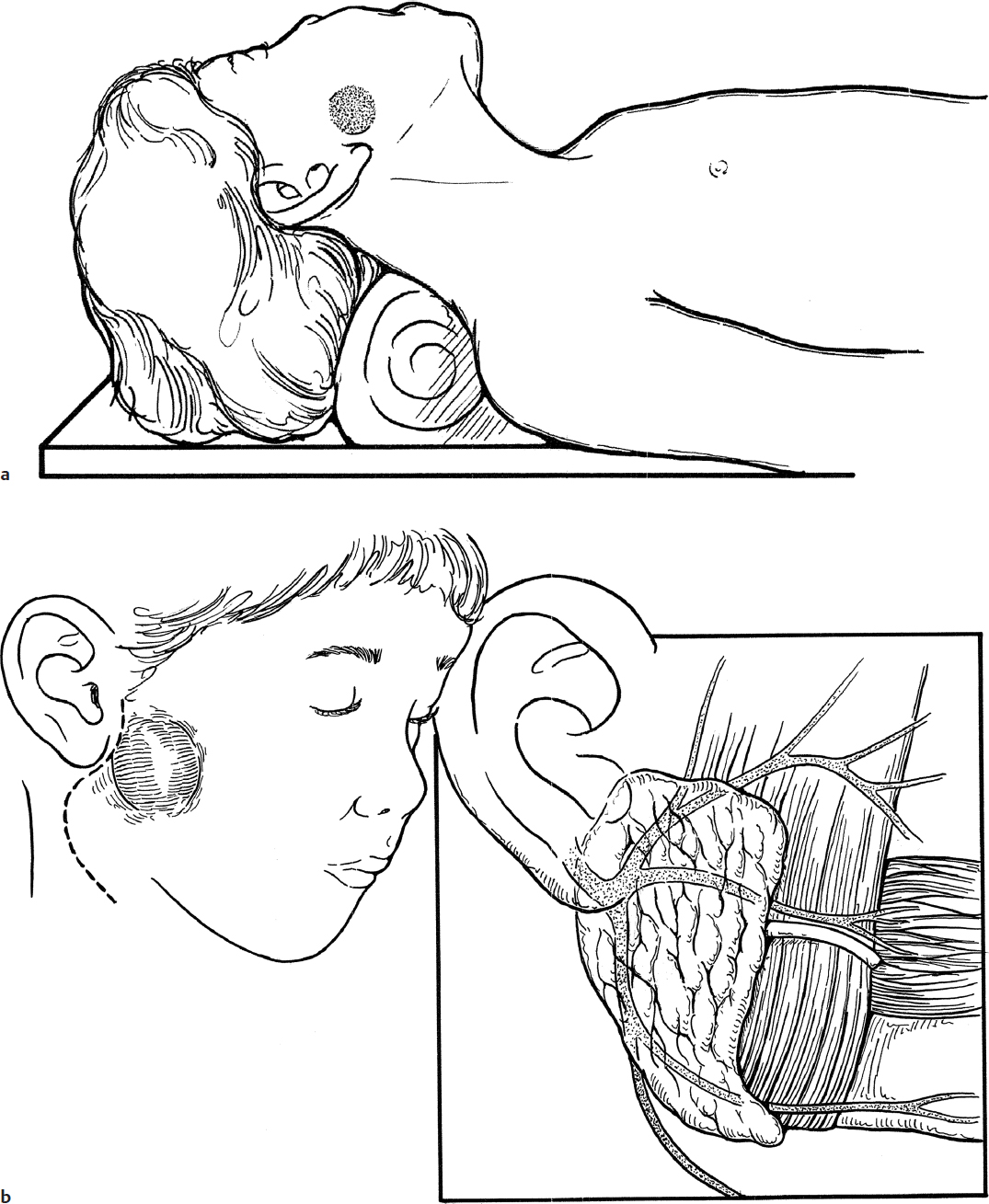
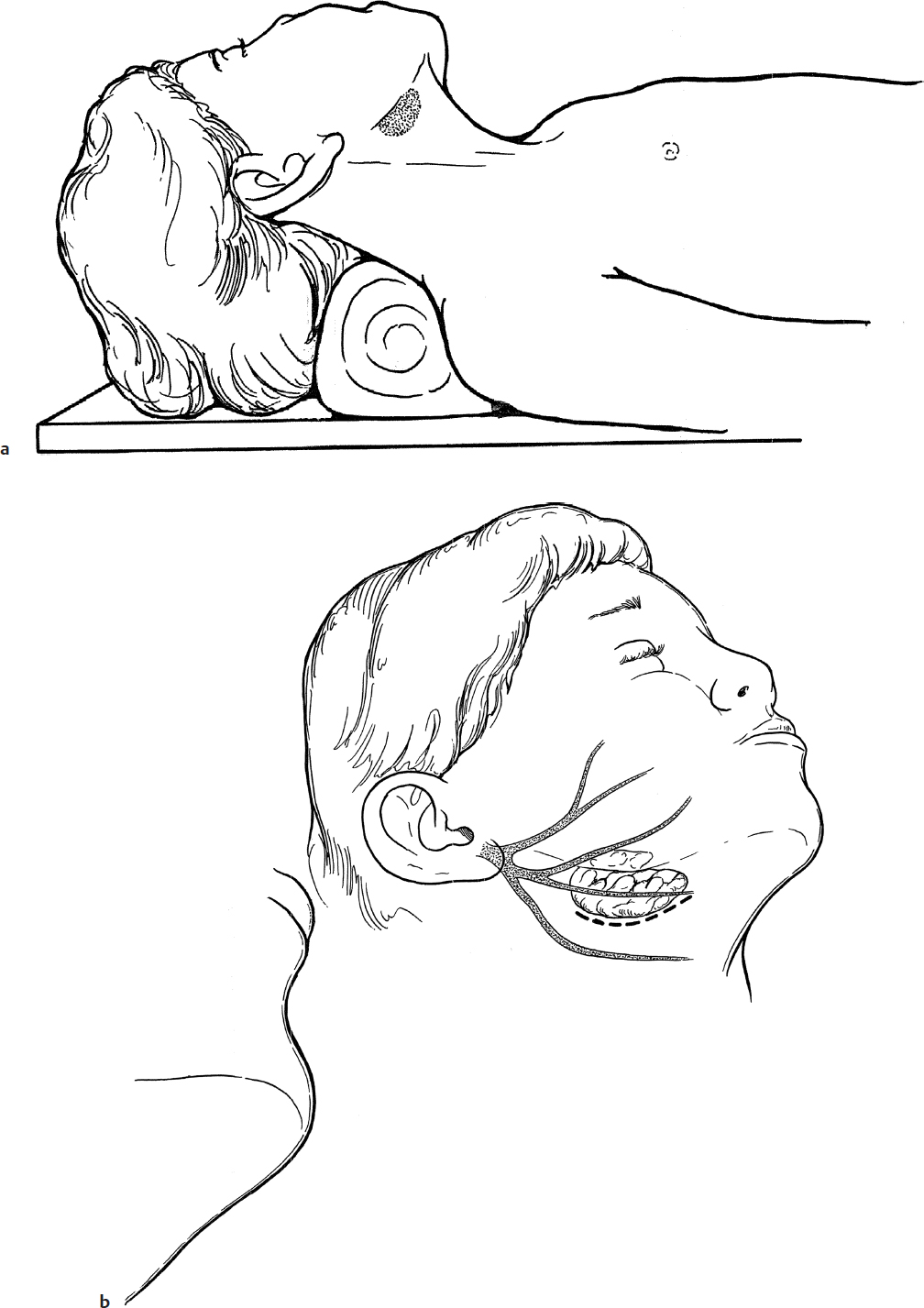
2. The patient is positioned on a shoulder roll with the neck slightly hyperextended and the head turned to the opposite side (Fig. 29.2a).
3. An incision is made starting in the preauricular line in front of the tragus. This is curved around the ear lobe, over the mastoid process, and continued onto the neck sufficiently below the mandible to avoid the marginal mandibular branch of the facial nerve (Fig. 29.2b,c).
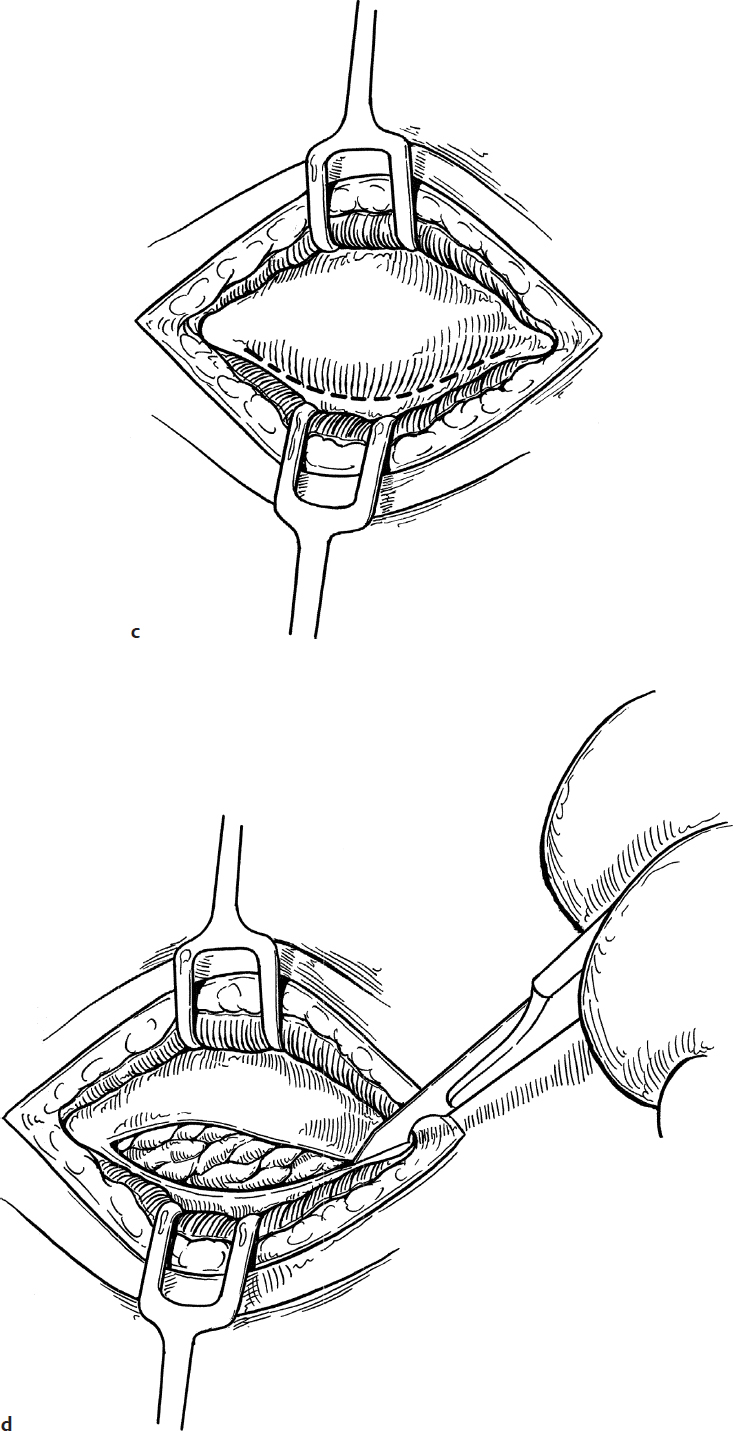
4. The skin flap overlying the parotid gland is elevated with a scissors anteriorly in the plane of subcutaneous fat (Fig. 29.2d). The ear lobule is retracted posteriorly with a 2-0 silk suture. This exposes the parotid gland fascia over the gland (Fig. 29.2e).
5. The superficial fascia between the parotid gland and the sternocleidomastoid muscle is cut with a scissors (Fig. 29.2f).
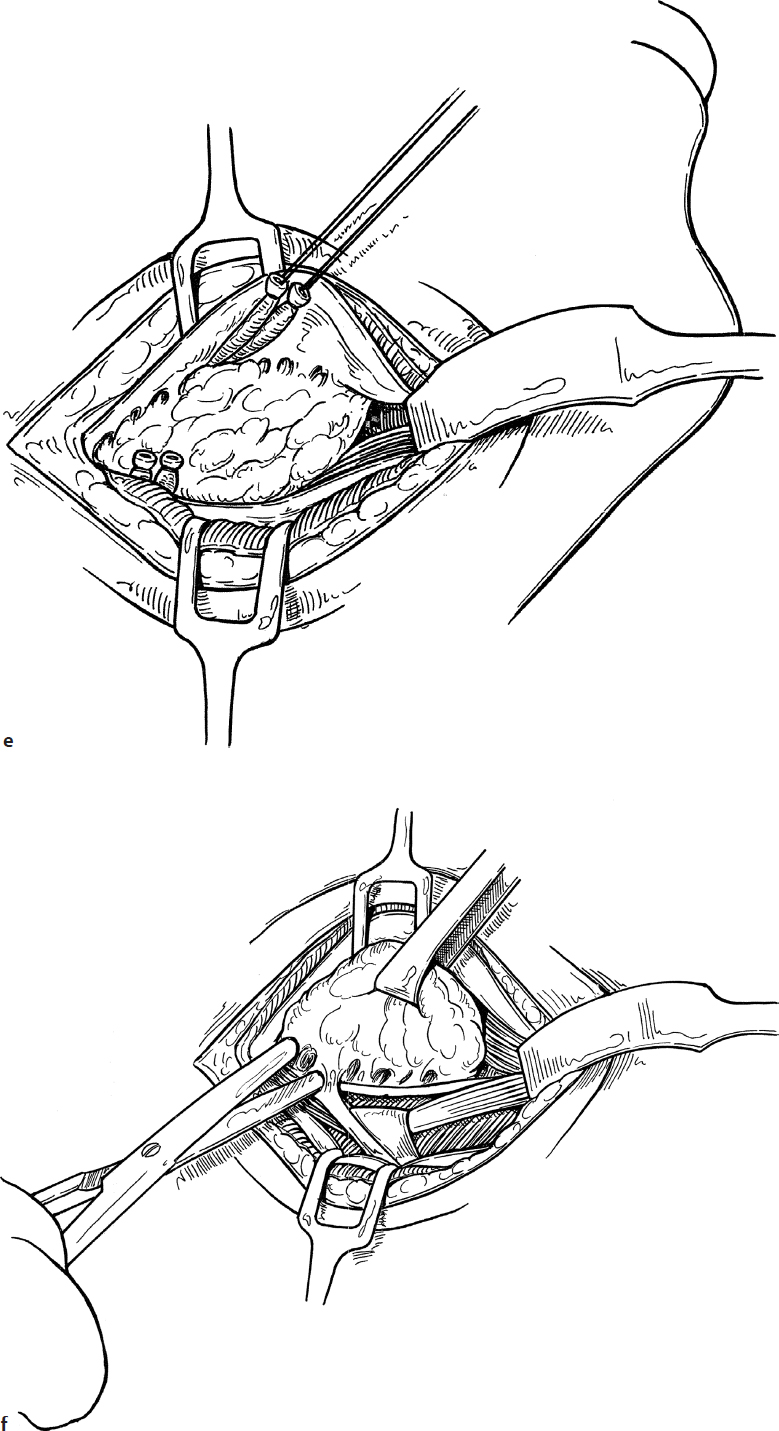
6. Dissection along the anterior and inferior surface of the cartilaginous external auditory canal is carried out with a clamp spreading in the direction of the facial nerve (Fig. 29.2g).
7. As the parotid gland is retracted forward, the facial nerve is stretched across the line of dissection and can be found in the groove between the mastoid tip and the bony ear canal (Fig. 29.2g). The facial nerve in the child is more superficial than in an adult and the usually described bony and cartilaginous landmarks for finding the nerve in adults rarely apply in the child (Fig. 29.2h).
8. As the parotid gland is reflected forward, the facial nerve can often be detected with a gentle fingertip as it enters the gland from the stylomastoid foramen.
9. Sufficient care and time should be taken to find the trunk of the nerve before any further dissection of the parotid gland is carried out.
10. Once the glistening white facial nerve trunk is found, its presence should be confirmed by testing with a facial nerve stimulator (Fig. 29.2i).
11. Dissection is then carried out by using a clamp over the nerve. While elevating and opening the clamp to lift the parotid tissue from the facial nerve, the parotid tissue is cut with a knife or scissors. The nerve is kept in view at all times (Fig. 29.2j).
12. Once the nerve trunk, bifurcation, and branches beyond the mass are dissected free, the parotid tissue between the areas over the nerve is released by either blunt or sharp dissection (Fig. 29.2k).
13. The mass is then removed with a cuff of normal parotid gland.
14. If the parotid duct is exposed, it should be ligated to prevent leak of saliva (Fig. 29.2l).
15. No attempt is made to remove all remaining parotid tissue such as that in the region of the zygomatic temporal branch or tail of the parotid unless it is involved in the disease process.
16. When a mass or diseased tissue is present in the deep lobe of the parotid gland, this tissue is removed by sharp dissection from the masseter muscle as the branches of the facial nerve are gently retracted out of the way (Fig. 29.2l).
17. The branches or main trunk of the facial nerve are again tested to confirm integrity, and the wound is closed with 3-0 chromic in the subcutaneous tissue and 4-0 interrupted subcuticular chromic in the skin (Fig. 29.2m).
18. A Jackson-Pratt drain is placed in the wound and brought out inferiorly for suction drainage (Fig. 29.2n). Suction drains work well to prevent hematoma formation but can create a noticeable depression in the region of the excised gland. The drain is removed in 24 to 36 hours.
Complications
1. Facial nerve injury
2. Gustatory sweating (Frey’s syndrome)
3. Salivary fistula