Salivary Duct Surgery and Sialorrhea Surgery
Chronic sialorrhea is a significant social problem that makes it difficult for children to participate in group activities (e.g., play groups and school).
28-1 Parotid Duct Ligation
Introduction
Parotid duct ligation reduces salivary production and causes atrophy of the gland.
Indications
Parotid duct ligation is performed in neuromuscularly impaired children to help control drooling. The indications for the operation are based on the history and observance of drooling that is a problem both for the child and for his caregiver. It is usually performed bilaterally and simultaneously with either bilateral submandibular gland excision or bilateral submandibular duct ligation. Submandibular gland excision is described in Section 29-1.
Preoperative Evaluation
Preoperative radiographic studies are not helpful.
Operative Technique
1. Parotid duct ligation is performed utilizing general nasotracheal anesthesia. This provides good oral exposure.
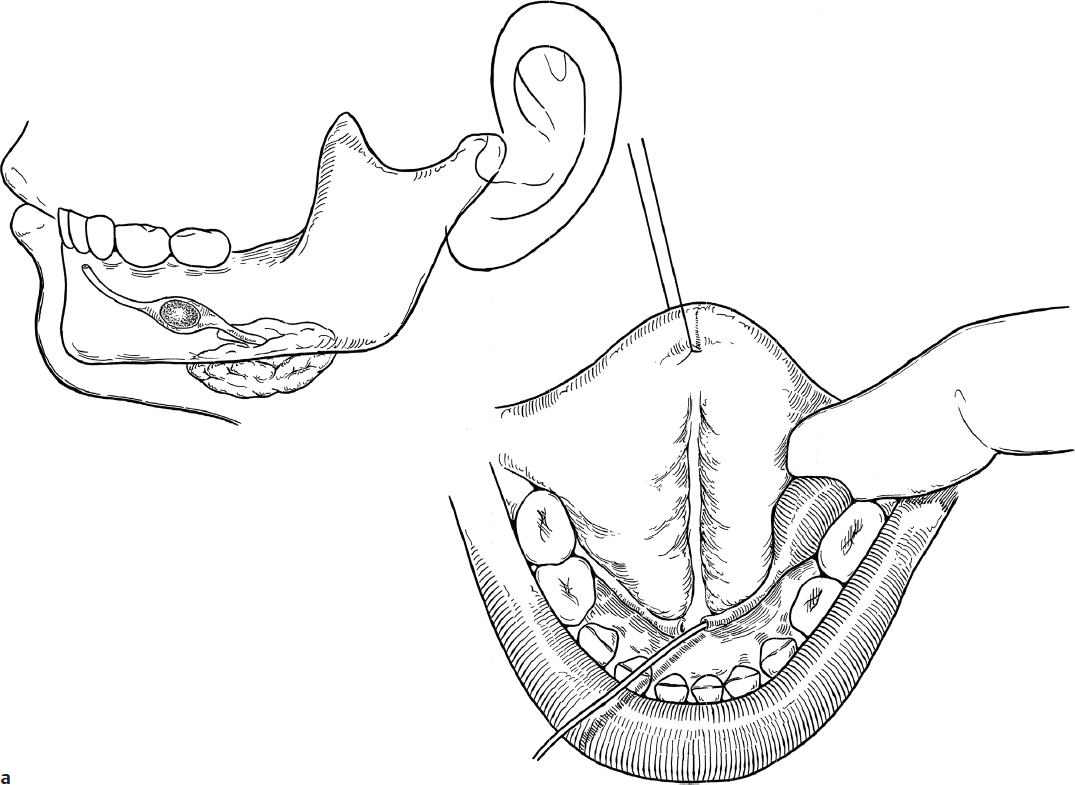
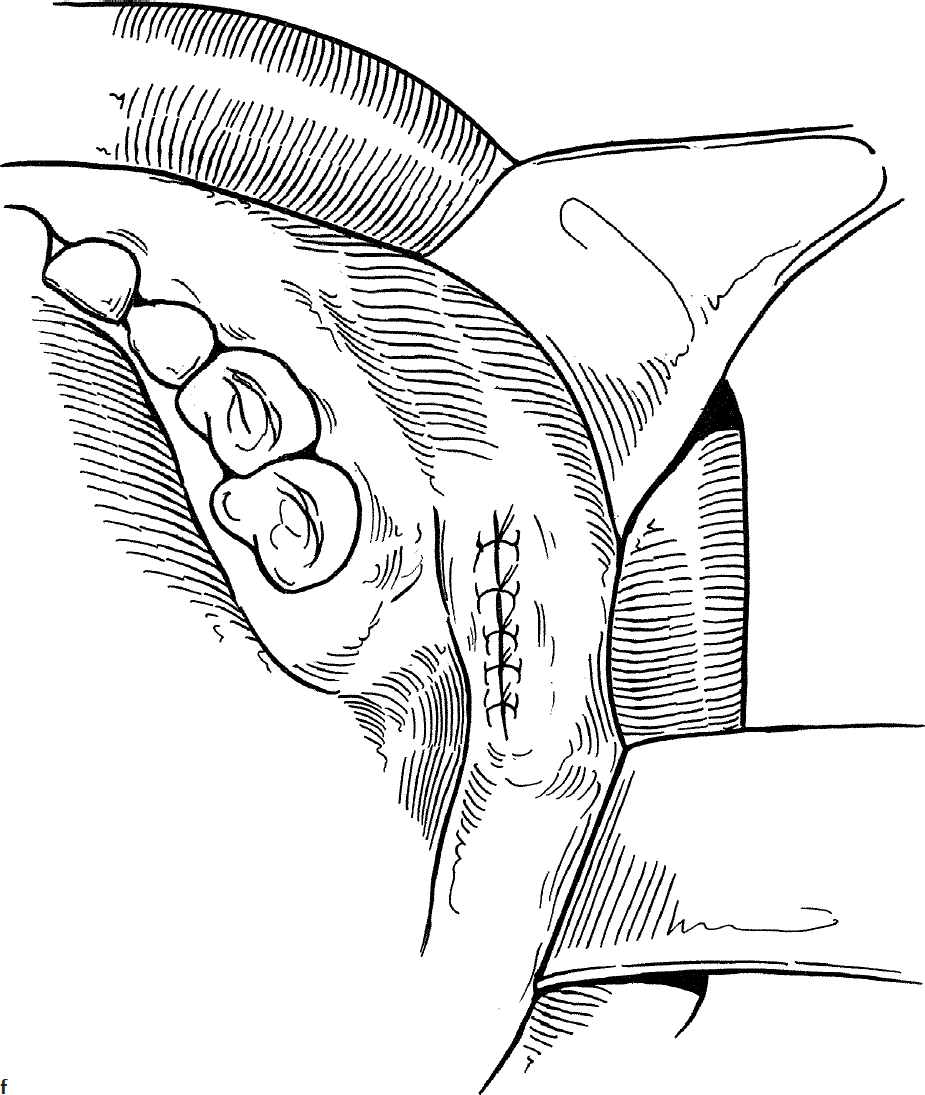
2. A lacrimal probe is inserted into the parotid duct to stabilize the papilla (Fig. 28.1a). One percent lidocaine with 1:1000,000 epinephrine is injected into the mucosa surrounding the papilla.
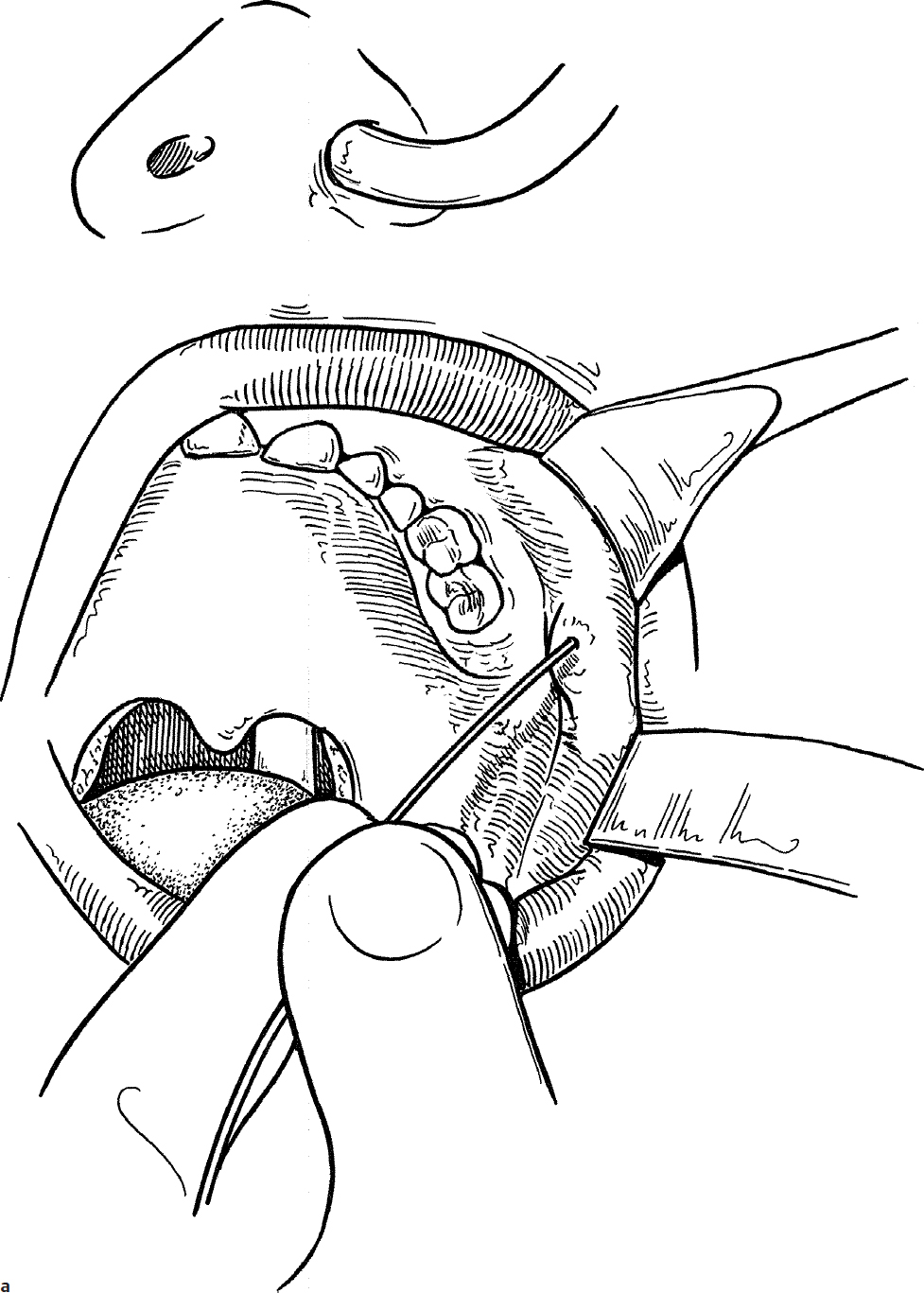
3. An elliptical incision is made around the papilla (Fig. 28.1b).
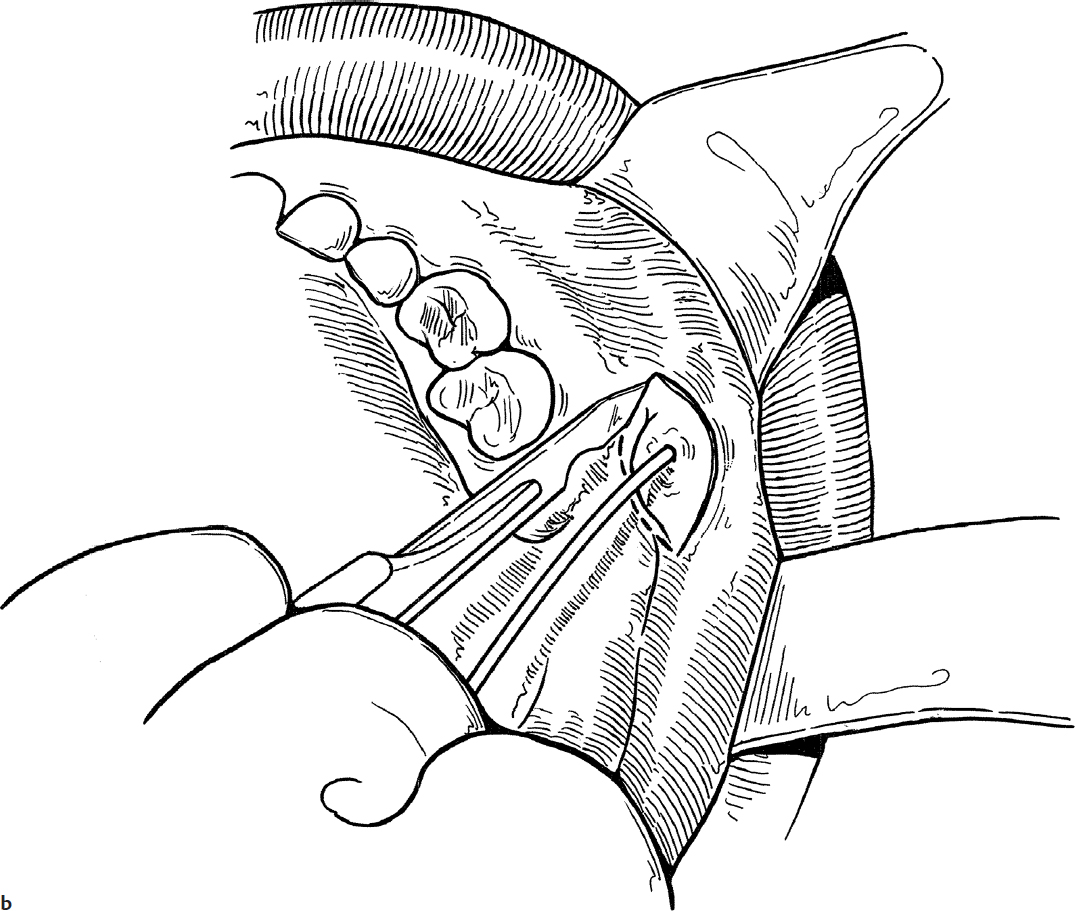
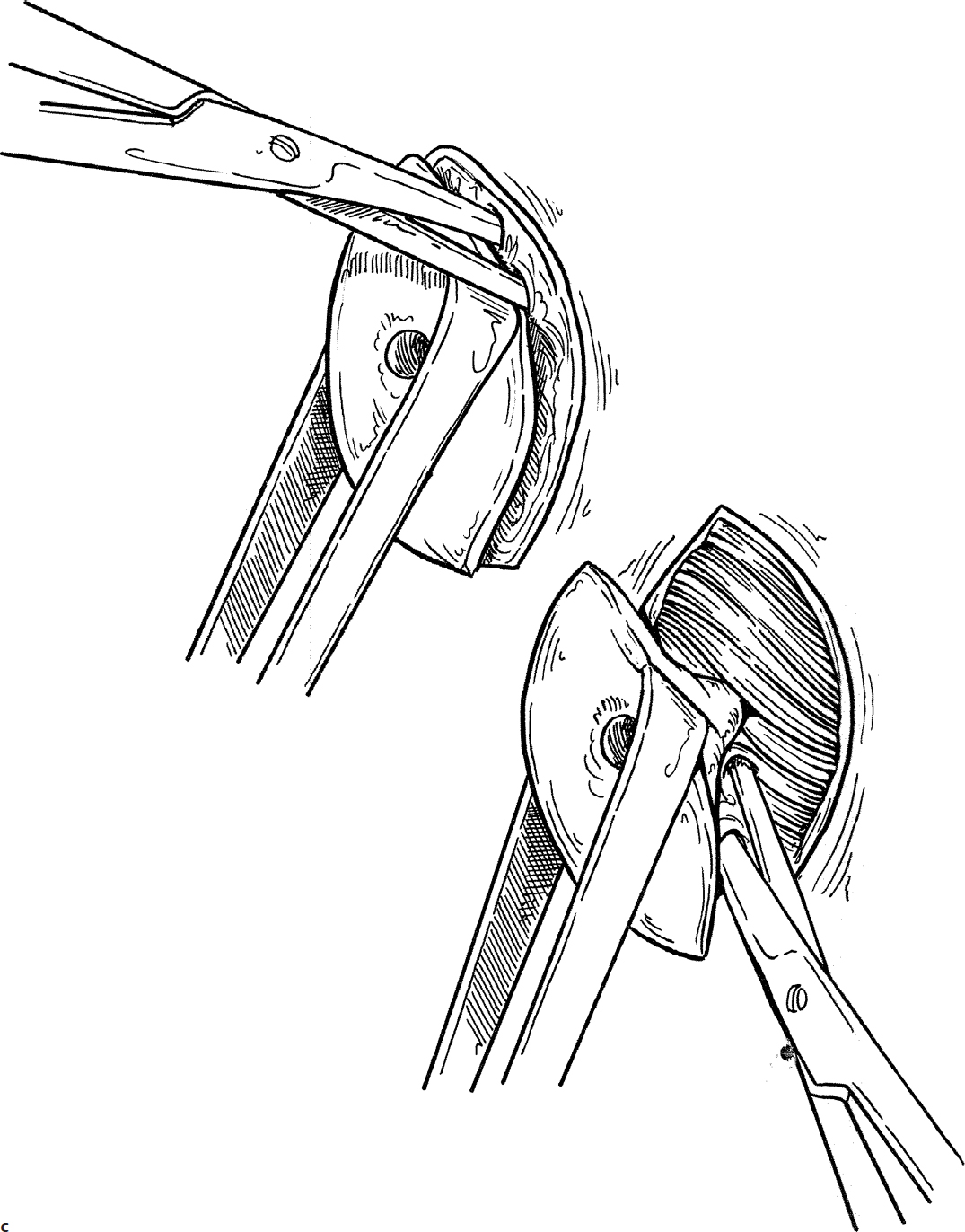
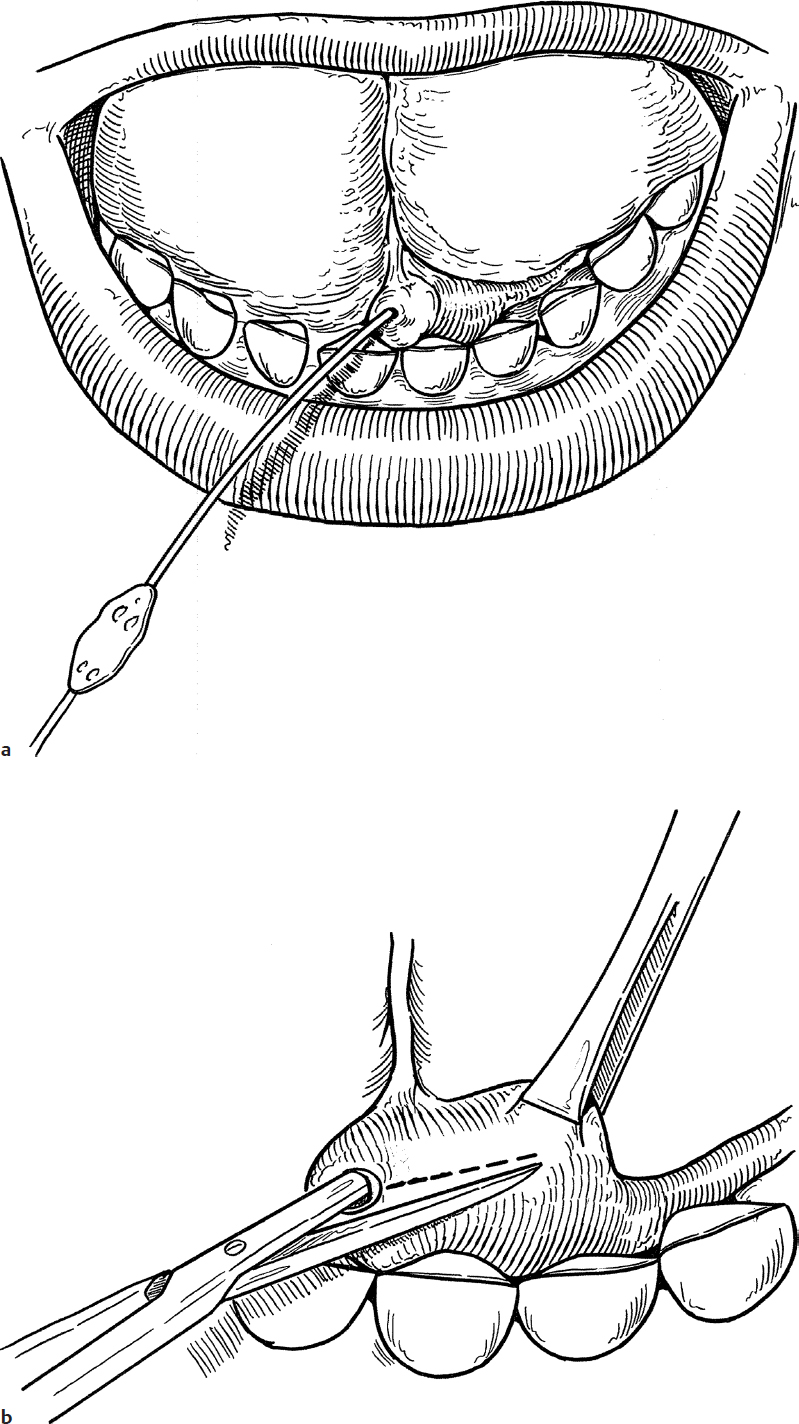
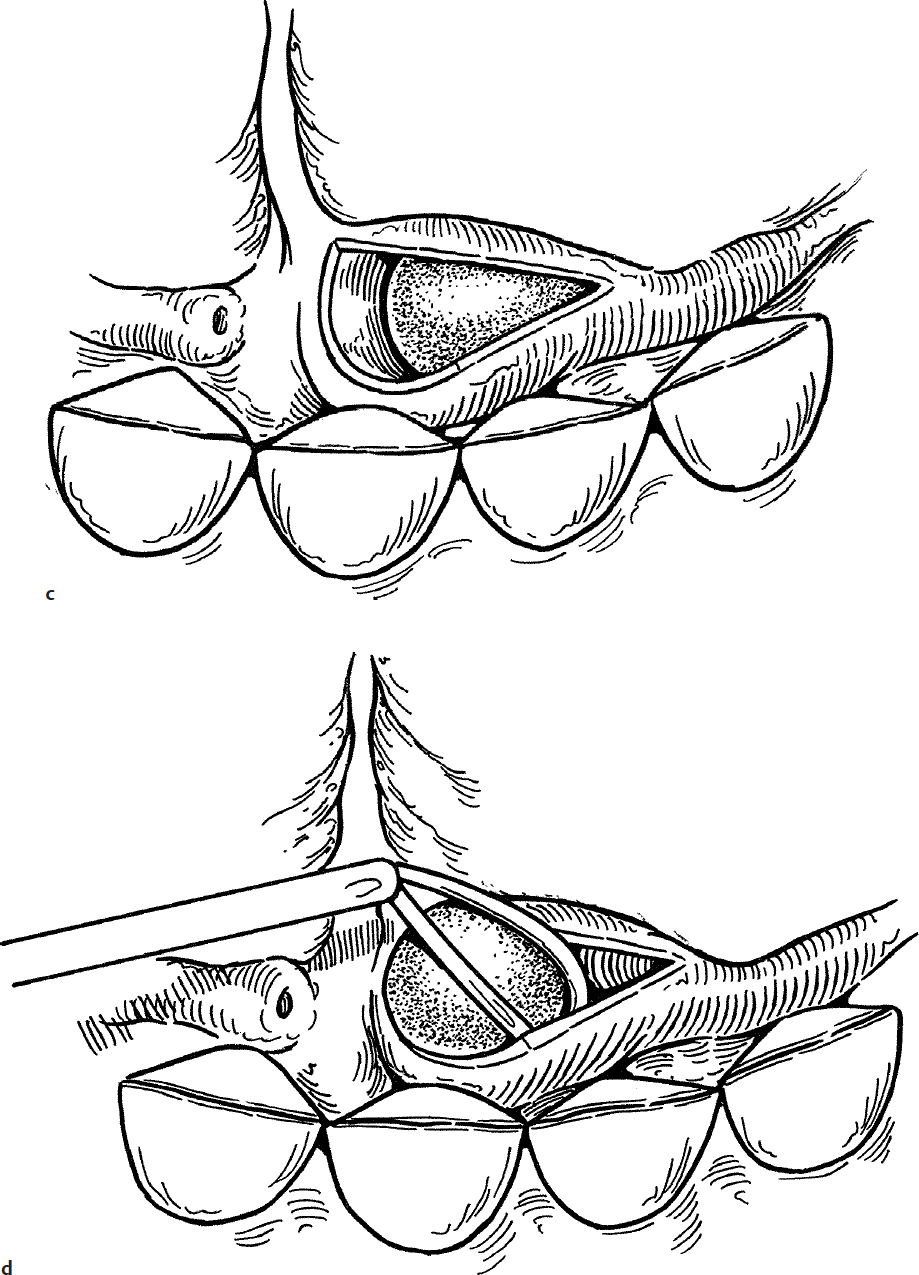
4. The papilla is grasped with a clamp and traction is placed on the duct while dissecting the duct free from surrounding tissue with a scissors (Fig. 28.1c).
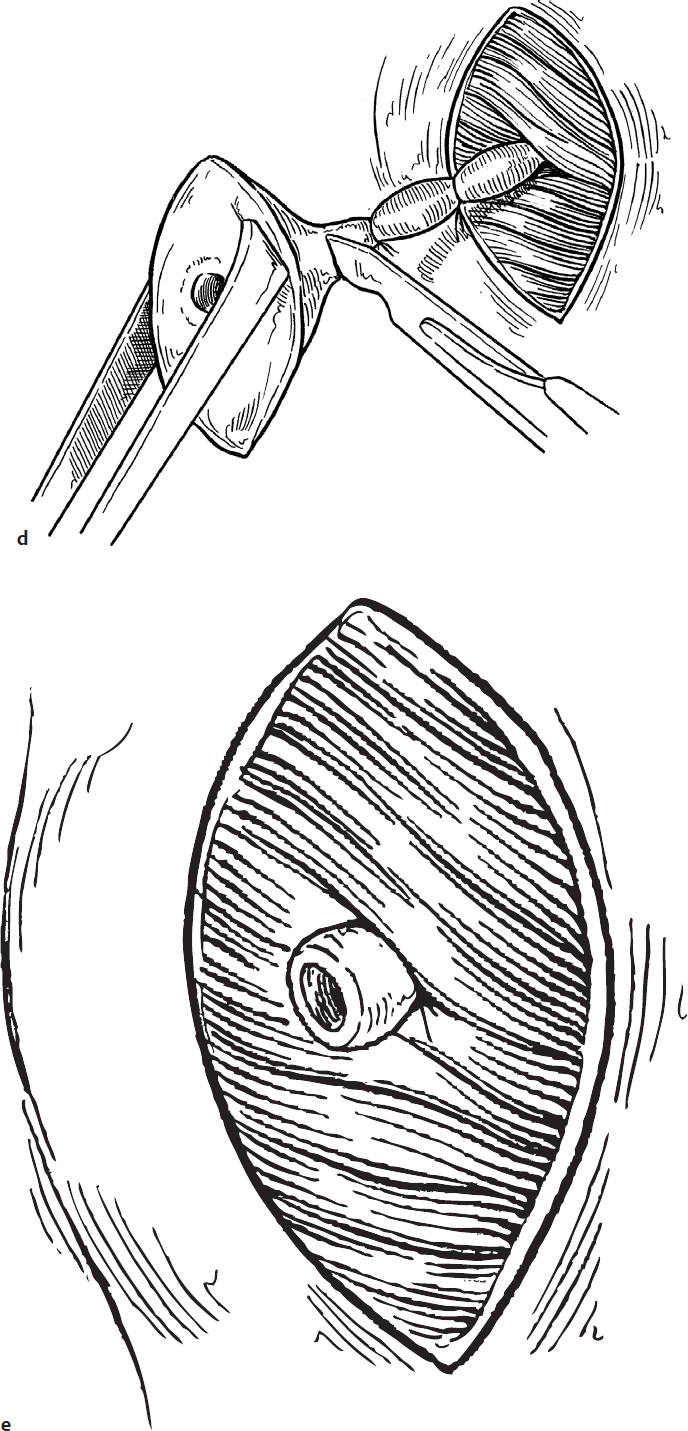
5. The duct is ligated twice with 3-0 silk suture and the papillary mucosa is excised by transecting the distal portion of the duct (Fig. 28.1d).
6. The duct is allowed to retract into the soft tissue of the cheek (Fig. 28.1e) and the oral mucosa is sutured loosely with 3-0 chromic suture (Fig. 28.1f).
Complications
Temporary painful parotid swelling.
28-2 Removal of Distal Salivary Duct Stones (Submandibular and Parotid)
Introduction
Salivary duct stones usually present with acute painful swelling of the involved gland. Some degree of bacterial infection from chronic stasis is often present.
Indications
Removal of salivary duct stones is indicated in cases of chronic or intermittent salivary gland swelling secondary to a ductal stone.
Preoperative Evaluation
Inspection of the duct in the oral cavity may reveal a turbid discharge. The stone usually can be palpated by passing the index finger along the course of the duct intraorally. Standard radiographic films are rarely helpful because salivary duct stones are usually not calcified. Sialography or magnetic resonance imaging (MRI) may be useful to demonstrate the position of the stone but usually are not necessary.
Operative Technique
1. Stones near the papilla of the submandibular gland are removed utilizing general anesthesia and nasotracheal intubation to provide optimal intraoral exposure.
2. The duct is dilated with lacrimal probes (Fig. 28.2a).
3. The duct is cut by placing one blade of a sharp-pointed scissors in the dilated duct and closing the blades to open the duct in a slitlike manner (Fig. 28.2b,c).
4. The stone is expressed from the duct or removed with a curette (Fig. 28.2d).
5. The ductal incision is not closed. Salivary flow will keep this new, larger orifice open.
6. Stones near the orifice of the parotid duct are treated in the same fashion.
Complications
Stricture of the duct.
28-3 Removal of Submandibular Duct Stones (Proximal)
Introduction
Salivary duct stones usually present with acute painful swelling of the involved gland. Some degree of bacterial infection from chronic stasis is often present.
Indications
The presence of a salivary duct stone causing swelling and/or infection of the involved gland is the indication for surgical removal.
Preoperative Evaluation
Inspection of the duct in the oral cavity may reveal a turbid discharge. The stone usually can be palpated by passing the index finger along the course of the duct intraorally.
Standard radiographic studies are rarely helpful because salivary duct stones are usually not calcified. Sialography or magnetic resonance imaging (MRI) may be useful to demonstrate the position of the stone but usually are not necessary.
Operative Technique
1. Submandibular duct stones are removed utilizing general anesthesia and nasotracheal intubation for maximum exposure.
2. With a lacrimal probe in the duct and a finger in the floor of the mouth, the stone is located by palpation (Fig. 28.3a).
3. A silk suture is passed around the duct proximal to the stone to prevent the stone from slipping back into the gland (Fig. 28.3b).
4. The portion of the duct containing the stone is opened with a knife and the stone is removed (Fig. 28.3b,c).
5. The mucosal incision is closed loosely with 4-0 interrupted chromic sutures. It is not necessary to suture the duct since the obstruction has been relieved and attempts at closure of the duct can cause stenosis (Fig. 28.3d).
6. Alternatively, sialendoscopy could be utilized to facilitate stone removal after submandibular duct dilation as needed.
7. Submandibular duct stones that are deep within the proximal portion of the ductal system should be removed by resection of the involved gland (see Section 29-1).
Complications
Stricture of the submandibular duct.