Purpose
To study safety of children’s glasses in rural China, where fear that glasses harm vision is an important barrier for families and policy makers.
Design
Exploratory analysis from a cluster-randomized, investigator-masked, controlled trial.
Methods
Among primary schools (n = 252) in western China, children were randomized by school to 1 of 3 interventions: free glasses provided in class, vouchers for free glasses at a local facility, or glasses prescriptions only (Control group). The main outcome of this analysis is uncorrected visual acuity after 8 months, adjusted for baseline acuity.
Results
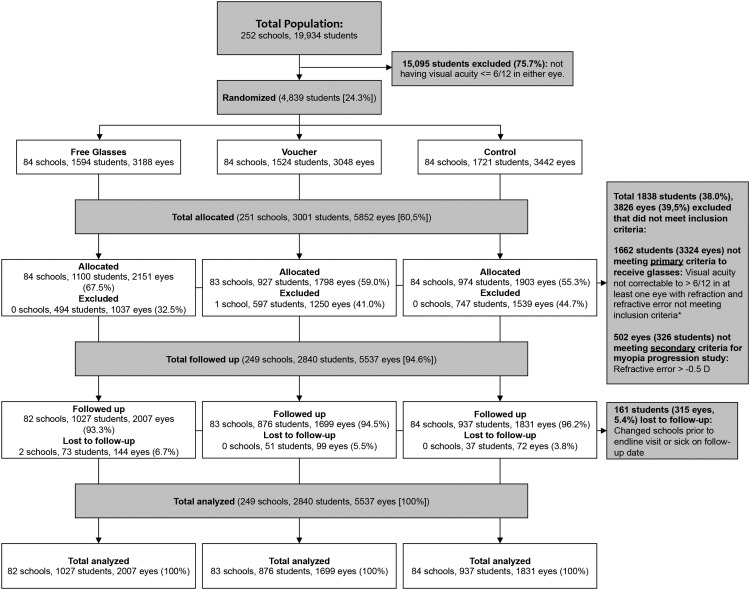
Among 19 934 children randomly selected for screening, 5852 myopic (spherical equivalent refractive error ≤−0.5 diopters) eyes of 3001 children (14.7%, mean age 10.5 years) had VA ≤6/12 without glasses correctable to >6/12 with glasses, and were eligible. Among these, 1903 (32.5%), 1798 (30.7%), and 2151 (36.8%) were randomized to Control, Voucher, and Free Glasses, respectively. Intention-to-treat analyses were performed on all 1831 (96.2%), 1699 (94.5%), and 2007 (93.3%) eyes of children with follow-up in Control, Voucher, and Free Glasses groups. Final visual acuity for eyes of children in the treatment groups (Free Glasses and Voucher) was significantly better than for Control children, adjusting only for baseline visual acuity (difference of 0.023 logMAR units [0.23 vision chart lines, 95% CI: 0.03, 0.43]) or for other baseline factors as well (0.025 logMAR units [0.25 lines, 95% CI 0.04, 0.45]).
Conclusion
We found no evidence that spectacles promote decline in uncorrected vision with aging among children.
Some half of all disability among children in the developing world is due to poor vision. The leading and most readily treated cause of children’s visual impairment (visual acuity [VA] <6/18) is refractive error, affecting 12.8 million children aged 5–15 years worldwide, half of whom live in China. Chinese children, for whom uncorrected refractive error accounts for 90% of visual impairment, have among the world’s highest rates of myopia (nearsightedness). Uncorrected refractive error is associated with worse self-reported visual function among children, and provision of accurate spectacles improves children’s functioning and educational outcomes. Spectacles provide an inexpensive and highly effective treatment for refractive error.
Despite the high prevalence and impact of children’s refractive error in rural China, rates of spectacle ownership and wear remain as low as 15% among those needing them. Studies in China and elsewhere suggest that a major reason for this is the perception among children, parents, and teachers that glasses wear harms children’s vision by worsening myopia. Concerns about the safety of glasses wear for children also influences policy makers. Government Health and Education Bureau websites in China may explicitly advise that children’s glasses wear leads to vision problems, or fail to recommend glasses as a treatment for myopia owing to safety concerns.
It is known that accurately measured glasses improve the corrected VA, but the concern among many laypersons in China is that wearing glasses will eventually worsen a child’s uncorrected VA, increasing dependence on their wear. It is this latter effect of glasses on the uncorrected vision that is not known. Previous small studies have been inconclusive on the effect of glasses wear on refractive power, and have not compared wear of glasses with nonwear, or directly reported effects on VA.
We carried out a large, cluster-randomized, population-based trial on the educational impact of providing spectacles to children with refractive error in rural China. We now report an exploratory, intention-to-treat analysis of the impact of assignment to receive access to free spectacles on uncorrected (without glasses) VA over the course of a school year, approximately 8 months.
Methods
The protocol for this study was approved in full by Institutional Review Boards at Stanford University (Palo Alto, California, USA) and the Zhongshan Ophthalmic Center of Sun Yat-Sen University (ZOC, Guangzhou, China). Permission was received from local Boards of Education in each region and from the principals of all schools. The principles of the Declaration of Helsinki were followed throughout. The original trial (Registration site: http://isrctn.org . Registration number: ISRCTN03252665) was designed to study the effect of providing free spectacles on children’s educational performance, and found that scores on a study-specific mathematic test were statistically significantly higher in the group receiving free spectacles compared to controls.
The hypothesis of the current exploratory analysis, based on our original trial data, is that provision of glasses would slow the decline in uncorrected VA expected to occur owing to increase in myopia (nearsightedness) commonly observed among children with aging. The primary outcome of the current analysis is uncorrected VA 8 months after provision of spectacles, adjusting for baseline VA. The choice of this outcome is based on the fact that uncorrected distance VA is expected to worsen with worsening myopia, and that vision itself, rather than refractive power, is the outcome of interest from the standpoint of disability and its alleviation. The methods of the original trial have been described previously and are provided here for reference.
Setting, Sampling, and Eligibility Criteria
The study was carried out in 2 nearby areas of western China: Tianshui prefecture, a poor area in Gansu, one of China’s poorest provinces, and Yulin prefecture, Shaanxi, a more affluent region in a middle-income province.
One school from each township in both prefectures was randomly selected from a list of all primary schools, and within each school, 1 class was randomly chosen in each of the fourth and fifth grades. For the original trial, all children at the 252 selected schools meeting the following criteria were eligible:
- •
Uncorrected (without glasses) VA ≤6/12 in either eye
- •
Refractive error as follows:
- ○
myopia ≤−0.75 diopters (D),
- ○
hyperopia ≥+2.00 D, or
- ○
astigmatism (nonspherical refractive error) ≥1.00 D
- ○
- •
VA could be improved to >6/12 in both eyes with glasses
In the current analysis, carried out by eye rather than child, all nonmyopic (refractive error >−0.5 D) eyes of eligible children were excluded ( Figure 1 ).
Questionnaires
At baseline (September 2012: beginning of the school year), enumerators administered questionnaires to children concerning their age, sex, glasses wear, awareness of their refractive status, boarding at school, and parental migration and education. A parental questionnaire asked about ownership of 13 selected items as an index of family wealth. Mathematics teachers were asked to state whether the blackboard was used for all teaching, most, about half, little, or none. At closeout (May–June 2013: end of the school year) children again filled out a questionnaire on glasses wear. Population density was calculated as the total population divided by total land area at the township level.
Assessment of Visual Acuity
Children underwent baseline VA screening at school by a nurse and staff assistant, previously trained by optometrists from ZOC. VA was tested separately for each eye without refractive correction at 4 meters using Early Treatment Diabetic Retinopathy Study (ETDRS) charts (Precision Vision, La Salle, Illinois, USA) in a well-lighted, indoor area. If the orientation of at least 4 of 5 optotypes on the 6/60 line was correctly identified, children were examined on the 6/30 line, on the 6/15 line, and then line by line to 6/3. If a line was failed, lines above were tested successively until the child identified 4 of 5 optotypes, with the VA for an eye defined as the lowest line read successfully. If the top line could not be read at 4 meters, the subject was tested as above at 1 meter, and the measured VA was divided by 4.
Refraction (Measurement of Glasses Power)
Children with uncorrected VA ≤6/12 in either eye underwent cycloplegia with up to 3 drops of cyclopentolate 1% and automated refraction (Topcon KR 8900; Tokyo, Japan) with subjective refinement by a refractionist, previously trained by experienced pediatric optometrists from ZOC.
Randomization and Interventions
This was a cluster-randomized, controlled trial, with schools as the clusters. In October 2012, after the baseline survey and vision screening but prior to refraction, eligible children were randomized by school to receive 1 of 3 interventions ( Figure 1 ):
- •
Free spectacles based on the child’s measured refractive power dispensed at school by the study optometrist (Free Glasses group, 84 schools);
- •
Vouchers bearing the child’s name, school name, and glasses prescription, exchangeable for free glasses at the local county hospital (distance from children’s township: range 1–105 km, median 30 km). Parents were responsible for paying transportation costs (Voucher group, 84 schools); or
- •
A glasses prescription and letter to the parents informing them of the refractive status of their child, with free glasses provided only at closeout, though this was not previously announced (Control group, 84 schools).
Schools were stratified by size, county, and number of children failing VA screening. We used R software (R Foundation for Statistical Computing, Vienna, Austria) to generate blocks of and randomly allocate schools within each block to the treatment arms.
Outcome Assessment
At closeout, VA was assessed using the protocol and vision chart described above. Spectacle wear was assessed through unannounced direct examinations on the same occasion. Children also described their own spectacle wear as “always,” “only for studying,” or “usually not worn.” Study personnel were masked to group assignment. Participants (students, parents, and teachers) and enumerators were not informed of either the overall design of the study or the explicit treatment arm assignment. During this visit, all children provided information on parental spectacle wear, and their own time spent out of doors and in near/middle distance work, important determinants of myopia progression.
Statistical Methods
Family wealth was calculated by summing the value, as reported in the China Rural Household Survey Yearbook (Department of Rural Surveys, National Bureau of Statistics of China, 2013), of items on the list of 13 owned by the family. Refractive power was defined throughout as the spherical equivalent, the spherical power plus half the cylindrical power.
Randomization groups were compared by intention-to-treat (ITT) analysis using multiple linear regression, with end-line uncorrected VA (logarithm of the minimal angle of resolution [logMAR]) as main outcome and intervention arms and baseline uncorrected VA as covariates. Other baseline variables were also investigated as predictors for final VA, with the final model including intervention arms and variables associated with baseline VA at P ≤ .20. Student and school were included in a random intercept model to adjust for the correlation between eyes of a student, between children in the same school, and between schools within the same randomization block. All analyses were performed using Stata 12.0 (StataCorp, College Station, Texas, USA), and SAS 9.3 (SAS Institute, Cary, North Carolina, USA).
Results
Among 19 934 children screened at 252 selected schools, 4839 (24.3%) failed VA screening and were randomized ( Figure 1 ). Of these, a total of 3177 children (65.7%) (6354 eyes) in 251 schools were eligible for allocation (VA improving with refraction). Among these, 5852 eyes (92.1%) of 3001 children (94.5%) were myopic; their baseline characteristics by treatment group are described in Table 1 .
| Characteristic | Control Group n =1903 a | Voucher Group n = 1798 a | Free Glasses Group N = 2151 a | Treatment Groups Combined (Voucher + Free) n = 3949 a | Missing Data (%) |
|---|---|---|---|---|---|
| Age (y) | 10.5 (1.1) | 10.5 (1.1) | 10.4 (1.1) | 10.5 (1.1) | 4 (0.07) |
| Male sex (%) | 948 (49.8) | 857 (47.7) | 1040 (48.4) | 1897 (48.0) | 0 (0) |
| Degree of myopia (diopters [D]): | 0 (0) | ||||
| ≤−0.5 and >−1.0 | 182 (9.6) | 206 (11.5) | 265 (12.3) | 471 (11.9) | |
| ≤−1.0 and >−1.5 | 489 (25.7) | 421 (23.4) | 537 (25.0) | 958 (24.3) | |
| ≤1.5 and >−2.0 | 383 (20.1) | 382 (21.2) | 437 (20.3) | 819 (20.7) | |
| ≤−2.0 | 849 (44.6) | 789 (43.9) | 912 (42.4) | 1701 (43.1) | |
| Baseline uncorrected visual acuity (logMAR) b | 0.6 (0.2) | 0.6 (0.2) | 0.6 (0.2) | 0.6 (0.2) | 0 (0) |
| Having glasses at baseline (%) c | 270 (14.2) | 262 (14.6) | 349 (16.2) | 611 (15.5) | 0 (0) |
| Total time spent in near work (hours/week) | 7.3 (3.6) | 7.5 (3.7) | 7.4 (3.6) | 7.5 (3.7) | 4 (0.07) |
| Total time spent in middle distance activities (hours/week) | 4.9 (4.2) | 5.2 (4.3) | 5.2 (4.5) | 5.2 (4.4) | 12 (0.21) |
| Total time spent in outdoor activities (hours/week) | 7.9 (3.8) | 8.0 (4.0) | 8.0 (4.1) | 8.0 (4.0) | 11 (0.20) |
| Boarding at school (%) | 442 (23.2) | 336 (18.7) | 546 (25.4) | 882 (22.4) | 3 (0.05) |
| One or more parents wearing glasses (%) | 676 (35.6) | 561 (32.7) | 780 (36.3) | 1372 (34.8) | 14 (0.25) |
| One or both parents with ≥12 years of education (%) | 384 (20.3) | 315 (17.7) | 490 (23.1) | 805 (20.7) | 58 (1.03) |
| Both parents out-migrated for work (%) | 207 (11.0) | 182 (10.2) | 195 (9.2) | 377 (9.6) | 52 (1.03) |
| Gansu residence (%) | 704 (37.0) | 647 (36.0) | 732 (34.0) | 1379 (34.9) | 0 (0) |
| Family wealth | 227 (4.04) | ||||
| Bottom tercile | 578 (32.0) | 619 (36.2) | 664 (31.9) | 1283 (33.8) | |
| Middle tercile | 659 (36.5) | 567 (33.1) | 643 (30.9) | 1210 (31.9) | |
| Top tercile | 567 (31.4) | 525 (30.7) | 775 (37.2) | 1300 (34.3) | |
| Blackboard use in class | 0 (0) | ||||
| Less than half of teaching | 498 (27.0) | 458 (26.6) | 824 (40.0) | 1282 (33.9) | |
| Half | 780 (42.3) | 700 (40.7) | 645 (31.3) | 1345 (35.6) | |
| More than half | 567 (30.7) | 563 (32.7) | 590 (28.7) | 1153 (30.5) | |
| Population density | 0 (0) | ||||
| 1st quartile | 450 (23.7) | 295 (16.4) | 598 (27.8) | 893 (22.6) | |
| 2nd quartile | 501 (26.3) | 484 (26.9) | 577 (26.8) | 1061 (26.9) | |
| 3rd quartile | 343 (18.0) | 467 (26.0) | 459 (21.3) | 926 (23.4) | |
| 4th quartile | 609 (32.0) | 552 (30.7) | 517 (24.1) | 1069 (27.1) |
a Data are presented as mean (SD) or number (%) unless otherwise stated.
b 0.1 change in logMAR indicates 1 line change on the vision chart.
c Defined as having glasses at school at baseline, having previously been told to bring them to school.
Intention-to-treat analyses were performed on all 1831 (96.2%), 1699 (94.5%), and 2007 (93.3%) eyes of children completing final VA assessment in the Control, Voucher, and Free Glasses groups ( Figure 1 ). Those with follow-up did not differ in any baseline variables compared to those without (data not shown).
Table 2 gives the baseline, end-line, and change in uncorrected VA by intervention group, as well as the effect on end-line VA adjusted for baseline VA of membership in the Voucher and Free Glasses groups compared with the Control group. When children in the 2 treatment groups (Free Glasses and Voucher) were pooled, their end-line VA adjusted for baseline VA was significantly better than for Control children by 0.023 (95% confidence interval [CI]: 0.003, 0.043) logMAR units (0.23 lines on the VA chart) ( Figure 2 ).
| Intervention Group | N | Mean Baseline Uncorrected LogMAR Visual Acuity (SD) | Mean End-Line Uncorrected LogMAR Visual Acuity (SD) | Unadjusted Change in LogMAR Visual Acuity (95% CI) | Effect of Interventions on End-Line Uncorrected Visual Acuity Adjusted for Baseline Acuity (95% CI) a |
|---|---|---|---|---|---|
| Total | 5537 | 0.59 (0.22) | 0.71 (0.21) | −0.12 a (−0.14, −0.10) | – |
| Control | 1831 | 0.60 (0.22) | 0.73 (0.21) | −0.13 a (−0.15, −0.10) | (Reference) |
| Voucher | 1699 | 0.58 (0.22) | 0.70 (0.21) | −0.11 a (−0.13, −0.09) | 0.028 a (0.004, 0.052) |
| Free Glasses | 2007 | 0.59 (0.21) | 0.71 (0.20) | −0.12 a (−0.14, −0.10) | 0.02 (−0.01, 0.04) |
| Treatment groups (Voucher + Free glasses) combined | 3706 | 0.58 (0.21) | 0.71 (0.20) | −0.11 a (−0.13, −0.10) | 0.023 a (0.003, 0.043) |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


