Purpose
To compare the effect of cohesive and dispersive ophthalmic viscosurgical device (OVD) on intraoperative rotational stability of the intraocular lens (IOL) with single-piece hydrophobic acrylate platform.
Design
Prospective, comparative study.
Methods
This institutional clinical study included 60 eyes of 60 patients who underwent phacoemulsifcation. The patients were equally divided into cohesive OVD (Healon GV; Abbott Medical Optics, Abbott Park, Illinois, USA) group and dispersive OVD (Viscoat; Alcon Laboratories, Fort Worth, Texas, USA) group. Image analysis from the captured digital image was used to measure intraoperative rotation of single-piece hydrophobic acrylate IOL (SA60AT or SA60NT) during OVD removal.
Results
Mean intraoperative rotation was 7.42 degrees ± 4.16 (standard deviation) in dispersive OVD group and 13.08 degrees ± 5.25 (standard deviation) in cohesive OVD group ( P < .001). Twenty-one cases (70%) maintained the alignment within 10 degrees during removal of OVD with dispersive OVD, while only 9 cases (30%) did so with cohesive OVD ( P = .005). Counterclockwise rotation was observed in 33% of the all cases.
Conclusions
This study showed that a significant amount of IOL rotation occurred during OVD removal. Intraoperative rotational stability of IOL was greater with Viscoat than with Healon GV.
The surgical outcome of modern cataract surgery has significantly improved with the introduction of small-incision phacoemulsification and other advanced technology. Therefore, many surgeons now advocate the concept of refractive cataract surgery, where the goal is to achieve minimal postoperative refractive error as well as visual recovery. Patients also expect fast visual recovery and better visual acuity without glasses after cataract surgery.
It has been reported that the theoretical or regression formula for intraocular lens (IOL) power calculation can predict postoperative refraction with high precision in most patients. But pre-existing astigmatism remains postoperatively with small-incision or micro-incision cataract surgery; thus patients with visually significant astigmatism will be dependent on spectacles for their distance vision after cataract surgery.
Approximately 15% to 20% of patients who undergo cataract surgery have more than 1.5 diopters of pre-existing astigmatism, which requires correction with glasses or contact lenses after surgery. Pre-existing astigmatism can be reduced during cataract surgery by adjusting the location, architecture, and length of the incision. Cataract surgery with additional incisional surgeries, including radial keratotomy and limbal relaxing incision, also can be considered.
Toric IOLs are advantageous over incisional surgeries in the predictability and stability of the refractive results. The optimal effect of the toric IOL depends on precise alignment and rotational stability of the IOL on the corneal astigmatic axis. Torsional misalignment of more than 10 degrees may induce 33% loss in the compensatory anti-astigmatic effect. A single-piece hydrophobic acrylic platform has been reported to show satisfactory postoperative torsional stability and is available as a toric IOL. However, unintended intraoperative rotation of the IOL may occur during phacoemulsification, especially during the removal of the ophthalmic viscosurgical device (OVD). Thus, the final alignment of these IOLs is indicated when the IOL is fully unfolded and all OVDs are removed from the anterior and posterior of the IOL. Manufacturers recommend the initial gross placement of the IOL with 5- to 10-degree counterclockwise misalignment, expecting clockwise repositioning of the IOL after OVD removal. But there have been no studies regarding the amount or direction of intraoperative rotation.
The aim of this study was to evaluate the intraoperative rotation of a single-piece hydrophobic acrylic IOL during OVD removal. We also compared the effect of cohesive and dispersive OVD on intraoperative rotational stability of these IOLs.
Methods
This prospective, randomized, institutional clinical study included 60 consecutive eyes of 60 patients who underwent cataract surgery. The patients were randomly divided into a cohesive OVD group and a dispersive OVD group. Exclusion criteria were corneal opacity, intraoperative posterior capsular tear, and poor mydriasis (<6.0 mm).
Preoperatively, white-to-white diameter and anterior chamber (AC) depth were measured using the Orbscan II system (Bausch & Lomb; Orbtek Inc, Salt Lake City, Utah, USA). Phacoemulsification and IOL implantation were performed with either a cohesive (1.4% sodium hyaluronate [Healon GV; Abbott Medical Optics, Abbott Park, Illinois, USA]) or dispersive (4% chondroitin sulfate–3% sodium hyaluronate [Viscoat; Alcon Laboratories, Fort Worth, Texas, USA]) OVD. All surgeries were performed by a single surgeon (J.Y.H.) using an Infiniti vision system phacoemulsification machine (Alcon Laboratories). Under topical anesthesia, a temporal 2.75-mm clear corneal incision was made with a slit knife. Capsulorhexis was intended to be 5.5 mm in size and was intact in all cases. Phaco chop technique was used in all cases. After phacoemulsification, the capsular bag and AC were filled with either the cohesive or dispersive OVD and a single-piece hydrophobic acrylic IOL (AcrySof SA60AT or SA60NT; Alcon Laboratories) was implanted into the capsular bag with an injector system through the clear corneal incision. The IOL was rotated to adjust it to the intended axis and allowed to fully unfold. After the IOL had fully unfolded, the OVD was completely removed from the anterior and posterior of the IOL with rock ‘n roll technique, in which an irrigation and aspiration hand-piece was placed on the anterior surface of the IOL and moved around the gently tilted optic edge of the IOL. Irrigation and aspiration parameters were 40 mL/min for flow rate and maximum 500 mm Hg for vacuum level.
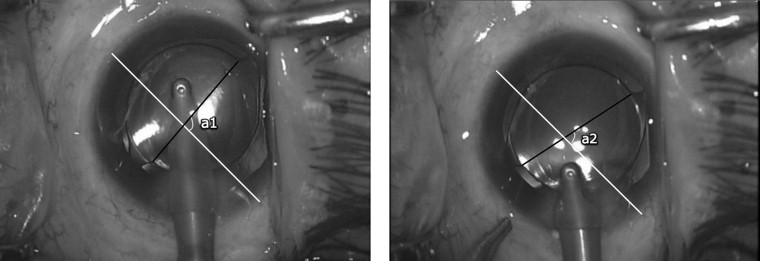
The rotation of the IOL during OVD removal was determined from the analysis of digital photographs. We adopted and modified the method described by Weinand and associates. Two digital photographs were captured from the recorded video just prior to and after OVD removal. A reference line was determined by connecting two critical details such as conjunctival vessels or certain points on the incision. Another line was determined by joining two details on the IOL (angulation points at the optic-haptic junction). The angle at the intersection of the 2 lines was measured and the difference in the angle between the two images was defined as the angle of rotation. Clockwise rotation was regarded as positive rotation in this study ( Figure ). Irrigation and aspiration time during OVD removal was recorded as well.
The angle of rotation, AC depth, white-to-white diameter, and irrigation and aspiration time were compared between the cohesive and dispersive OVD groups. SPSS software for Windows version 13.0 (SPSS Inc, Chicago, Illinois, USA) was used for statistical analysis with Student t test and χ 2 test. Any P value less than .05 was considered statistically significant.
Results
White-to-white diameter and AC depth were not significantly different between 2 OVD groups ( Table 1 ). The mean amount of intraoperative IOL rotation during OVD removal was 10.25 ± 5.50 degrees (0.4 to 22.4 degrees). Of the 60 cases, the angle of rotation was within 10 degrees only in 30 cases (50%) after OVD removal. There was a statistically significant difference in the angle of IOL rotation between the 2 groups. The angle was significantly smaller in the dispersive OVD group (7.42 ± 4.16 degrees vs 13.08 ± 5.25 degrees; P < .05, Student t test). Intraoperative rotation of IOL within 10 degrees was observed in 21 cases (70%) of the dispersive OVD group, but only in 9 cases (30%) of the cohesive group ( P = .005). Out of the 60 cases, 40 cases (67%) had clockwise rotation, while 20 (33%) showed counterclockwise rotation. There was no difference between the 2 OVD groups in the direction of rotation. The mean angle of clockwise rotation was 10.98 ± 5.60 degrees and that of counterclockwise rotation was 8.80 ± 5.12 degrees, showing no significant difference in the amount of rotation between the 2 directions. More than 15 degrees of clockwise rotation was observed in 8 cases with cohesive OVD and 1 case with dispersive OVD. Irrigation and aspiration times were longer with dispersive OVD than with cohesive OVD ( Table 2 ).
| Cohesive (n = 30) | Dispersive (n = 30) | P value a | |
|---|---|---|---|
| Age | 66.97 ± 9.25 | 69.77 ± 6.96 | .19 |
| WTW (mm) | 11.51 ± 0.52 | 11.50 ± 0.48 | .98 |
| ACD (mm) | 2.79 ± 0.31 | 2.80 ± 0.25 | .92 |
| Axial length (mm) | 23.68 ± 0.81 | 23.62 ± 1.23 | .84 |
| Cohesive (n = 30) | Dispersive (n = 30) | P value | |
|---|---|---|---|
| Mean rotational angle | |||
| (Mean ± SD) (degree) | 13.08 ± 5.25 | 7.42 ± 4.16 | < .001 a |
| Rotation within 10 degrees | 9/30 (30.0%) | 21/30 (70.0%) | .005 b |
| CW rotation | 22/30 (73.3%) | 18/30 (60.0%) | .410 b |
| (Mean ± SD) (degree) | (13.35 ± 5.37) | (8.07 ± 4.47) | |
| CCW rotation | 8/30 (26.7%) | 12/30 (40.0%) | .410 b |
| (Mean ± SD) (degree) | (12.34 ± 5.16) | (6.43 ± 3.16) | |
| I/A time | |||
| (Mean ± SD) (second) | 19.40 ± 5.28 | 50.77 ± 11.08 | < .001 a |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


