Role of Vision Screening in the Detection of Congenital or Early Acquired Cataracts
M. Millicent W. Peterseim
Pediatric cataract remains an important form of treatable childhood blindness and lifelong visual impairment. There are an estimated 200,000 children blind from cataract worldwide.1 Thus congenital cataract, as a treatable cause of visual handicap in childhood, is a priority of the global Vision 2020 initiative.2 Successful outcomes require the early recognition of infantile and congenital cataracts. Children are a vulnerable population because, unlike adults who note a loss of vision, children are usually unaware of and do not complain of their deficit. Detection of pediatric cataracts is carried out by caretakers and primary care providers as part of a general childhood health screen. Tools used by primary care givers range from observation of the eyes and visual function to acuity measurement. By necessity, these tools change as the child grows and develops. This chapter reviews the importance of screening and useful techniques in detection of childhood cataracts.
DETECTION IN INFANTS
Of primary concern is the detection of cataracts in infants because of the risk of devastating amblyopia resulting in a lifetime of visual impairment. Successful surgical repair and rehabilitation must be instituted early to allow development of normal vision. Significant lens opacity during the critical period of visual development results in poor vision and, in bilateral cases, sensory nystagmus that usually persists even after excellent surgical and restorative care. In visually significant newborn cases, cataract surgery within 6 weeks of birth produces the best outcome. Sensory nystagmus will develop if dense bilateral cataracts are not cleared before at least 3 months of age (see Chapter 6). Therefore, screening for pediatric cataract is imperative as part of the initial newborn as well as subsequent well-baby exams. A Swedish study found that 80% of congenital cataracts were detected when screening was performed in the hospital maternity ward, compared with 67% of cases when screening was deferred to the first well-baby check. Three children per year were operated on too late and thus missed the opportunity for good visual development in the future.3 Thus, it is important that newborns undergo screening for congenital cataracts within the first few days of life with subsequent screenings at a few weeks of age.
THE RED REFLEX TEST
The American Academy of Pediatrics (AAP) states that “red reflex testing is an essential component of the neonatal, infant, and child physical examination” and has published the practice pattern guidelines and techniques of this test. The AAP recommends all children undergo a red reflex assessment as a component of the eye evaluation in the newborn nursery and during all subsequent routine health supervision visits.4 The test should be performed in a darkened room (to maximize pupil dilation). The direct ophthalmoscope is focused on each pupil individually approximately 12 to 18 inches away from the eyes. As a second stage, both eyes are viewed simultaneously approximately 3 feet away with the child focusing on the ophthalmoscope light (Fig. 4.1). The red reflex seen in each eye individually should be bright reddish-yellow in lightly pigmented eyes or grey in darkly pigmented, brown-eyed patients, and identical in both eyes. Dark spots in the red reflex that do not move with a blink, a blunted dull red reflex, lack of a red reflex, a white reflex, or asymmetry of the reflexes (Bruckner test) are all indications for referral (Fig. 4.2). The See Red card is available to provide reference for this test (Fig. 4.3).5
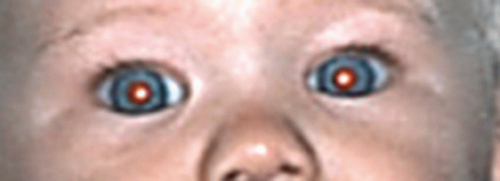 Figure 4.1. Symmetric red reflexes in an infant. |
Any question as to the red reflex test findings should warrant expedited referral. Historically, poor communication between eye care providers and primary care doctors has hampered the effectiveness of vision screening.6 Effective communication between the primary care giver and ophthalmic health professionals is critical to the success of this approach and the care of the child.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


