Fig. 1
Transoral robotic surgery endoscopes. Depicts the dual camera system of the robotic endoscopes which provides a three-dimensional high definition display. The endoscope on the left maintains a diameter of 12 mm and the right maintains 8.5 mm diameter
The arms on each side of the central endoscope are equipped with robotic instruments. With well over 30 types of instrument designs, identifying the optimal surgical instrument can sometimes be laborious. Instruments are broadly categorized by their diameter and by their function. The first generation of robotic instruments maintained 8 mm outer diameter, which included a right-angled jointed instrument. However, newer instruments now maintain a smaller 5 mm outer diameter. The 5 mm instruments are recommended within the tight spacing of the pharynx and larynx. The newer 5 mm instruments are also designed with a wristed joint to allow for improved reach and dexterity.
The instrument function can be categorized as either cutting or retracting. Given the specialized tissue of the larynx and airway, the cutting energy options should be reviewed. The most common cutting energy instrument is the Bovie monopolar cautery, which can be delivered by either a spatula or hooked tip. TORS is routinely performed with the use of the spatula tip. Bipolar cautery instruments were previously only available in 8 mm diameter, but a 5 mm bipolar cautery forceps has recently been made available for clinical use. Bipolar will likely become adapted within TORS procedures as clinical experience collects.
Harmonic scalpel (Ethicon Endo-Surgery, Inc., Cincinnati, Ohio, USA) robotic instrument is available in both 8 mm and 5 mm diameters; however, complexity in energy delivery has prevented the harmonic scalpel from obtaining the same degree of wristed angulation that is typical of the other robotic instruments. As such, its description has to date been limited to blood vessel control within cervical compartment surgeries. With improved degrees of motion, the harmonic scalpel will likely have a larger role in laryngeal TORS, specifically endoscopic ligation of the superior laryngeal artery.
Laser integrated instruments make up the last group of cutting instruments. Intuitive Surgical only offers the thulium laser fiber delivery as an integrated robotic instrument. While a positive experience with the thulium laser in the larynx and pharynx has been described [2, 3], popular use is still limited. This underutilization may be related to relative unfamiliarity with the thulium wavelength or perhaps from the capital requirement of purchasing a new thulium laser system in addition to the robotic system. Third party laser adapters have allowed for the conversion of standard retracting instruments into robotic-assisted CO2 laser delivery systems. Specifically, Lumenis Inc. (Yokneam, Israel) producing the FiberLase Robotic Drop–in Guide and OmniGuide Inc (Cambridge, Massachusetts, USA) producing the FlexGuide Ultra provide CO2 fiber delivery instruments. Overall, both systems provide a flexible fiber guide that is fitted for robotic graspers (recommended instrument is the 5 mm needle driver) (See Fig. 2). The fiber can be delivered and removed as needed throughout each procedure. On a practical level, both systems offer individual differences that can be considered when comparing the laser system.
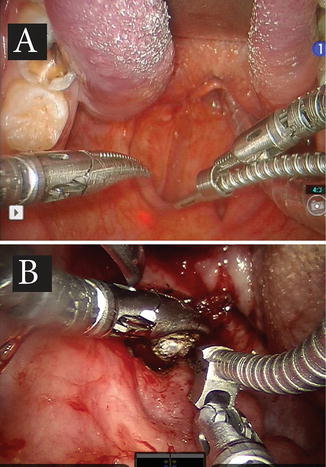
Fig. 2
CO2 laser flexible fiber delivery systems. Third party CO2 laser delivery systems are shown. Lumenis provided Fiberlase system (a) and Omniguide provided FlexGuide system (b) are adapted to robotic needle drivers. One of the main differences between the systems is the presence of the aiming HeNe beam of the Fiberlase (a) system
The most distinct difference between the Omniguide and FiberLase by Lumenis is the laser energy dispersion. Energy dispersion is seen when the laser spot widens as the tip of the fiber is moved away from the target. The energy dispersion reduces the final laser power density or cutting efficiency. However, the energy dispersion also helps coagulate small diameter (~1 mm) blood vessels. OmniGuide laser energy typically has a wider field of energy dispersion than the FiberLase. This increased dispersion can be seen as an advantage for either system depending on surgeon preference. A more dispersed energy beam will coagulate more effectively while a more focused energy beam will offer a more precise incision line. Another difference between the two fiber laser systems is that the FiberLase provides a HeNe aiming beam, similar to standard articulated armed CO2 delivery systems. Both robotic-assisted CO2 laser systems have been reported with good early clinical experience [4, 5]. Table 1 reviews the general advantages and disadvantages of the available cutting instruments.
Table 1
Summary of strengths and limitations of TORS cutting instrumentation
Surgical precision | Thermal damage | Blood vessel coagulation | |
|---|---|---|---|
Flexible fiber CO2 laser | ++++ | ++ | ++ |
Thulium laser | ++ | +++ | +++ |
Electrocautery | + | ++++ | ++++ |
Cold knife | ++++ | – | – |
TORS and Microsuspension Laryngoscopy
A TORS approach for laryngeal and airway surgery is typically suggested as an alternative to standard microsuspension Direct Laryngoscopy (mDL) with either laser or cold knife surgery. The same contraindications that have been well described for mDL surgery are applicable for laryngeal TORS. Specifically, potential patients must:
Maintain overall health to undergo the strains of general anesthesia
Accept cervical spinal extension without vertebral precautions
Demonstrate acceptable mandibular excursion
When malignancy is present, the tumor must be amenable to endoscopic resection (e.g., an absence of vocal fold fixation)
Surgical risk profiles are similarly described between mDL and TORS, including but not limited to chipped teeth, tongue numbness, taste alterations, airway swelling, or bleeding. It is common for patients to undergo diagnostic mDL prior to proceeding to laryngeal TORS so that the patients may have an understanding of the requirements and risk profile.
However, there are also noticeable advantages that TORS offers over the mDL approach. The high-definition wide-angle endoscope of the robotic system offers a superior visualization of the operative field. As demonstrated (See Fig. 3), TORS can offer wide-field visualization of the entire operative field while still being able to magnify the area of interest. The difference in field of view can be minimal in the case of lesions confined to the glottis, yet larger lesions which extend beyond the anatomic boundaries of the glottis typically exceed the view of standard direct laryngoscopes. The robotic visualization is also enhanced by a three-dimensional (3D) display which is superior to that of binocular display of the operative microscopes. Adjusting the operative view is also improved with the robotic system. The surgeon-controlled endoscope (by way of the console foot pedal) can rapidly recenter the surgical view without effort or disruption to the surgical momentum which is in contrast to the surgical disruption required for microscope readjustments.
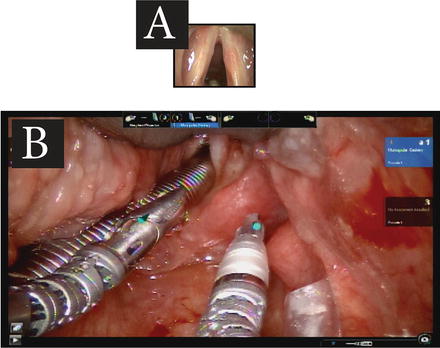
Fig. 3
Comparative views of Microdirect laryngoscopy and TORS. Direct laryngoscopes provide microscopic magnification of lesions of the glottis (a). Robotic endoscopes can provide similar magnified view of the glottis while still providing wide-field view of the supraglottis, hypopharynx, and oropharynx in the same frame (b). The small blue cones seen in b are produced by the teaching console of the dual console robotic system
TORS also provides improvement in surgical dexterity. With degrees of freedom at the instrument wrist, angled surgical motion can achieve improved direction of retraction and cutting over that of the static directionality of long-handled mDL instruments. Additionally, the long-handled mDL instruments enhances physiologic hand tremor. However, the movement scaling of the robotic system provides a tremor-free surgical action along with graded motion. Finally, the placement of the cutting instrument in the field of surgery (as in the spatula bovie arms) provides a two-handed surgical experience. In contrast, when an articulated-arm laser system is used, one hand is required for beam aiming leaving only one surgical instrument in the surgical field.
Laryngeal TORS approach also adds improvement with education and training of future surgeons. mDL procedures can prove to be challenging to observe with frequent microscope adjustments and limited field of view. In comparison, the wide field view of TORS will typically provide an improved observing experience for students and surgeons-in-training. The newer (Si, Xi) generations of the robotic system provide an additional layer of training with the dual console. Now, surgeons-in-training can observe the surgical procedures from the exact perspective of the operative surgeon. The observing personnel can also move the surgical controls along with the surgery as a “rehearsal.” When the nonoperating console moves the surgical controls, visual markers are displayed across the digital displays as blue pointers (See Fig. 3b). When the surgeon-in-training achieves sufficient experience, operative control of the robotic instruments may be alternated between the two consoles, between the two surgeons, so that initial surgical experiences may be provided in a controlled manner (See Fig. 4). Finally, the computer-based simulator of the robotic system allows for standardized skills training and objective trainee metrics. In all, the transition from mDL to TORS approach when appropriate may allow for improved training of the next generation of laryngeal surgeons.
Fig. 4
Training surgical simulation. As the surgeon-in-training is seated at the operative console (left), example screen shot of surgical simulation is displayed (upper right). Objective training measures (lower right) are also recorded and are available for supervising surgeon review
Clinical Applications
From the technical advantages, a number of robotic-assisted surgical approaches have been adapted to the larynx and airway. This chapter will now discuss more frequently described applications. The surgical approaches described require extensive training. Endoscopic laryngeal and airway surgery experience will also clearly enhance the transition to endoscopic robotic surgery. An “inside-out” understating of laryngeal neurovascular anatomy is critical in order to avoid major surgical complications [6]. These approaches also require specialized head and neck training for the robotic system concentrating on transoral exposure and transoral placement of instrumentation to access the larynx and airway [7]. Additionally, robotic surgery programs should allow surgeons the appropriate time to progress through the expected learning curve [8] and should plan cases more proximal in the head and neck, such as the palatine tonsillar fossa, reserving laryngeal robotic surgery for only the experienced robotic surgeon.
Supraglottic Laryngectomy
For many tumors of the supraglottis primary surgical resection may offer an excellent treatment option. While the most common malignancy of the supraglottis is squamous cell carcinoma, surgical resection can also be commonly recommended for other tumors of the supraglottis such as nerve sheath tumors [9], paragangliomas [10], and carcinoid tumors [11].
Operative Technique
The operative technique for TORS supraglottic laryngectomy parallels the techniques for endoscopic CO2 laser supraglottic laryngectomy [12]. Variations in technique are required based on the anatomic location and extent of tumor progression. Recommendations for surgical excision have therefore been divided according to the classification scheme of the European Laryngological Society (ELS) (See Fig. 5) [13].
Fig. 5
European Laryngological Society (ELS) Supraglottic laryngectomy classifications. Depicts the European Laryngological Society (ELS) classification scheme for endoscopic supraglottic laryngectomy. The classification scheme, though designed for endoscopic CO2 laser supraglottic resections, has successfully been adapted to TORS laryngectomy
Exposure is obtained utilizing the operative pharyngoscope of choice. The authors use the Laryngeal Advanced Retraction System (LARS) pharyngoscope. Resections limited to the suprahyoid epiglottis can be exposed with a tongue blade fitted into the vallecula (See Fig. 6a). The remaining resections including deeper portions of the supraglottis, such as the aryepiglottic fold or false vocal folds, should be first exposed with a laryngeal (long, narrow width) tongue blade fitted at the petiole (See Fig. 3b). With this configuration, the posterior-most boundaries may be incised first before blood can obscure the dependent portions of the operative field. If needed, the epiglottis can then be released from retraction with minor adjustments to the pharyngoscope for epiglottic or vallecular incisions.
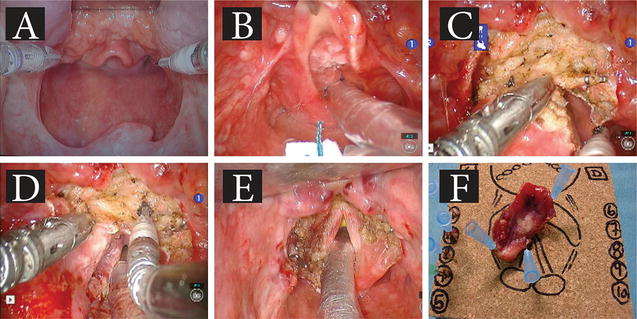
Fig. 6
TORS medial supraglottic laryngectomy with resection of preepiglottic space (type IIIa). The robotic-assisted images display the critical steps of type IIIa supraglottic laryngectomy. (a) demonstrates initial placement of operative pharyngoscope (LARS system used here) exposing the vallecula and larynx. (b) shows the T2 squamous cell carcinoma on the laryngeal surface of the epiglottis. (c) is following surgical clipping of the right superior laryngeal vessels. Following which, (d) transects the vessels and resects the preepiglottic space fat, extending inferiorly to the level of the laryngeal ventricles. (e) demonstrates the post-resection larynx with minimal glottal edema. (f) shows en-bloc resection specimen oriented for accurate pathologic analysis; intraoperative margin assessment is performed by the additional specimens (seen with the number labels on the left side of figure)
A “Limited Excision” (type I) supraglottic laryngectomy entails excision of small superficial tumors on the free border of the epiglottis, the aryepiglottic fold, the arytenoids, or the ventricular fold or any other part of the supraglottis. In cases of small and superficial T1 tumors of the laryngeal surface of the epiglottis located above the hyoid bone, the resection includes half of the suprahyoid epiglottis. This procedure is a “Limited Medial” supraglottic laryngectomy without resection of the preepiglottic space (type IIa).
“Medial” supraglottic laryngectomy without resection of the preepiglottic space (type IIb) should be applied for T1 tumors of the laryngeal surface of the epiglottis extending below the hyoid bone. In these cases, a total epiglottectomy is performed. The incision line goes through the preepiglottic space without its complete excision. The pharyngoepiglottic, aryepiglottic, and ventricular folds are preserved.
The resection of T1 or T2 tumors extending to the petiole of the epiglottis must include the preepiglottic space. This procedure is the “Medial supraglottic laryngectomy with Resection of the Preepiglottic Space” (type IIIa) (See Fig. 6). The incision is guided along the valleculae until the hyoid bone is reached. The incision line moves caudally from the hyoid bone toward the thyrohyoid membrane until the upper border of the thyroid cartilage is exposed. From this point, the whole entity of the preepiglottic space is removed along the inner surface of the lamina of the thyroid cartilage together with the epiglottis, toward the anterior commissure of the vocal folds.
T1–T2 tumors of the infrahyoid epiglottis extending to the ventricular fold can be resected with the same technique (type IIIb). The ventricular folds can be completely dissected from the thyroid cartilage along the inner surface toward the ventricle of Morgagni.
In cases of tumors of the aryepitglottic fold (also known as marginal tumors) with possible extension to the ventricular folds, the resection includes the free edge of the epiglottis, the three folds’ region, and the ventricular fold. This procedure is the “Lateral” supraglottic laryngectomy (type IVa).
The “Lateral supraglottic laryngectomy with Arytenoid Resection” (type IVb) was proposed in case of extension to the mobile arytenoids; the arytenoid is included in the resection. The resection may include the inner or medial and anterior part of the pyriform sinus.
As much as possible en bloc resections should be performed. The specimen is examined, but frozen sections are typically taken from the laryngeal margins after tumor resection. Tracheostomy is not a recommended portion of this surgery. Cervical nodal basins also require intervention, either through selective neck dissections or through sentinel lymph node biopsy [14]. The details of these procedures are beyond the scope of this text but should be part of the surgical plan. The authors routinely perform the neck surgeries during the same anesthetic administration as the robotic-assisted resection.
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


