Fig. 1
Lymphatic tongue base obstruction (endoscopic view)
The preoperative diagnostic approach is basically the same for all potential surgeries of sleep related breathing disorders: history, conventional ENT examination, awake fiberendoscopy (Naso Pharyngo Laryngoscopy), biometrics (Body Mass Index [BMI], Neck Circumference, Tonsils Grading 0 to IV, Mallampati–Friedman Scoring I to IV, Cormack and Lehane Scoring), psychometrics (Epworth Sleepiness Scale, Cognitive Functions Test Battery, Anxiety and Depression Scales, Electronic Reactometry), Imaging (basically Panorex® & Lateral Cephalogram), Quality of Life SF36 questionnaire. In this particular group of patients Sleep Endoscopy and Neck CT or MRI proved to be a very useful additional set of investigations for better defining soft tissue collapsing pattern during sleep and relative obstructing mass composition (lymphatic tissue vs. muscle) in base of tongue (BOT) bulging (Fig. 2).
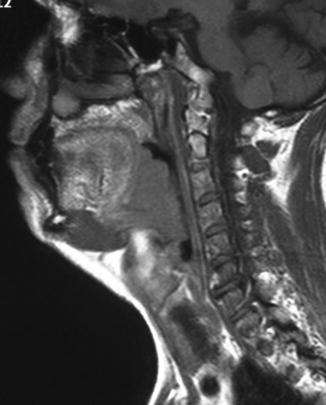
Fig. 2
Lymphatic tongue base obstruction (MRI pre-op)
In many cases patients are referred to surgery after continuous positive airway pressure (CPAP) not acceptance or drop-out. In a significant number of patients TORS is proposed as a revision procedure after previous surgery failure. Additional complaints commonly reported by most of the patients are related to BOT enlargement; foreign body sensation in the throat, swallowing difficulties and chronic cough.
Associated nasal obstructive problems as well as palate and tonsil disproportionate anatomy may be treated in the same time of TORS with additional surgical steps in the same operation (multilevel surgery including nose reconstruction and Expansion Sphincter Pharyngoplasty according to Pang & Tucker Woodson, that replaced in our experience the more classical but less effective uvulopalatopharyngoplasty).
Cardiovascular and neuropsychological comorbidities usually related to OSAHS must be accurately evaluated by the anaesthesiological team, in order to rule out too high risk patients or properly managing the more complex cases. Obesity is the most common dysmetabolic condition encountered as well as arterial hypertension and metabolic syndrome. It is worth to mention that TORS for OSAHS is a BMI sensitive procedure. In patients with BMI > 30 the expected success rate decreases along with the BMI increasing. Specific technical features of TORS for OSAHS must be pointed out. Airway problems are very probable in induction as well as in post-op survey for OSAHS patients.
1.
Difficult intubation facilities are always at disposal, and endoscopic assisted intubation was necessary in 80 % of our cases, not different from Literature figures.
2.
Especially for most severe OSAHS cases a safety tracheostomy is strongly recommended for post-op ventilation assistance, moreover if nose and oropharynx are operated in the same time. One more key point for tracheostomy is the degree of difficulty in case of reintubation for airway problems or post-op bleeding. The present policy of our group is to discuss any single case with the anaesthesiological team and share the final decision about a planned tracheostomy, that is no more adopted in mild to moderate cases, without significant comorbidities, scheduled for a limited surgical treatment (tongue base and supraglottis without nose and/or palate) and expected to be easily reintubated if necessary. If required, tracheostomy is the first step of TORS. A specific study comparing conventional/incisional with dilatiative/percoutaneous is still running in our Institution. Preliminary unpublished data seem to favour the dilatative, more expensive but less aggressive and easy to perform out of the operating room in the patients’ preparation area. An additional advantage of tracheostomy to be stressed is a completely tube free surgical field during robotic procedure, very useful in case of very narrow pharynx. In our Institution post-op Protocols for severe OSAHS patients require routine tracheostomy. A prolonged post-op intubation inside the recovery room may be an alternative solution. We use to check the airway by fiberoptics in order to optimize the timing of tube removal, usually about few hours after the surgery, and in order to avoid the intubation induced edema, sometimes more prominent than postsurgical one.
Technique
Tongue base exposure is achieved in the standard TORS approach with a combination of tongue body traction with strong sutures and tongue body displacement by Storz® Davis Meyer Mouth Gag. A complete set of tongue blades of different sizes with integrated suction tubes (for smoke and blood) is of paramount importance. FK® Mouth Gag is available on the table but usually is not necessary for TBR in most cases but sometimes may be useful for SGP. A small size blade proved to be the most suitable tool in most cases, especially in the first steps of BOT approach. Cheek retraction by means of disposable auto-retaining retractors (Leone Orthodontics and Implantology®, Florence, Italy) is possible in order to gain more space laterally, especially for a better view of the 2nd surgeon for his manoeuvres. 12 mm 30° 3D scope (upward facing) is our preferred choice. If available 8 mm scope may be very interesting in particular cases (small interincisive distance, extreme macroglossia, etc.).
Only two robotic 5 mm Endo Wrist® arms are used for each patient: a Maryland Dissector 400143/420143 for grasping and dissection of tissues and a Monopolar Cautery with Spatula Tip 400142/400160 for dissection and coagulation. No clip placement is usually required, but in few special cases large vessel clipping proved to be very helpful. Sometimes additional haemostasis is provided by an insulated ball-end coagulation-suction tube Storz® Cat. 12067R at disposal. An insulated long blunt angled-tip bipolar forceps Storz® Cat. 842219 is of paramount importance for safe coagulation in the peripheral aspects of the surgical field. A bipolar Dessi’s coagulating device originally designed for FESS may be helpful as well. Two additional hands with a suction device type mini-Yankauer are offered by the assistant surgeon at the head of the patient. Tissue displacement for better surgical exposure, blood and smoke suctioning are the basic jobs of the assistant surgeon.
Some special remarks about specificity of OSAHS TORS may be discussed into detail:
The patient’s so-called supine “sniffing position” is preferred in order to achieve the best compromise for basic good exposure and possibility to apply all possibly required external manoeuvres of neck compression/ lateral displacement in order to enhance the exposure of different areas during the dissection.
1.
A single case customized combination of tongue base traction and properly selected mouth-gag blade length is the key for a really good exposure. It requires a correct amount of tongue base bulging into the surgical field for the best manipulation.
2.
In extremely huge tongue situations, the smallest Storz blade may allow a lateral inrolling of the tongue body margins. In this situation the operative arms introduction may be difficult. The use of a longer and wider blade is possible in order to sustain the lateral tongue body profiles, provided that a lower degree of tension of the tongue suture is set in order to allow a more posterior tongue base bulging.
3.
Repositioning of tongue blade may be rarely necessary and in our experience it would be considered as the last choice. Usually the shortest blade or the medium blades are very effective for completing tongue base as well as epiglottis procedures. If a second blade is to be inserted after first resection step, the new position must be checked in a very precise way in order to avoid losing the orientation.
4.
Only in few cases FK mouth gag proved to be crucial, especially for supraglottic exposure; it’s usually not necessary in tongue base exposure.
TORS approach in OSAHS surgery includes two different surgical procedures usually combined in the same patient [5–9]:
1.
Tongue Base Reduction (TBR)
2.
Supra Glotto Plasty (SGP)
Tongue base reduction (TBR): It’s basically a different application and a proper modification of the tongue base resection described by O’Malley and Coll. in 2006 [10]. The goal of TBR is to enlarge the oropharyngeal section in the anterior wall area as well as classically palatine tonsils removal and lateral pharyngoplasty address the more common lateral oropharyngeal wall obstruction. As in the lateral oropharyngeal wall, in tongue base area, there is surgically safe superficial layer composed of lymphoid tissue easy to remove and surgically dangerous deep muscular layer composed of muscles covering great vessels (lingual artery and its dorsal branches) and functionally crucial nerves (hypoglossus nerve and lingual nerve).
The end point of TBR may be probably achieved when the obtained surgical view shifts from a Cormack & Lehane Grade IV to a Grade II, or far less commonly, to a Grade I. In all but few cases lymphoid tissue as well as tongue base muscle must be removed in order to clear the so called Retrolingual Space or Posterior Airway Space (PAS).
The more lymphatic hyperplasia, the less muscular tissue violation. Conversely, if lingual tonsil is no more than a thin layer, a more aggressive muscular resection is required in order to get the Cormack & Lehane Grade II goal. The mean volume of removed tissue is of about 15 cc, but sometimes the overall volume may be over 50 cc. Surgical steps are quite standardized in a precise and may be logic sequence, and may be sequentially applied in most of the approached cases [11]:
1.




Midline split of the two lingual tonsils from foramen caecum down to identify epiglottic tip and vallecula. The section is carried out by Monopolar Cautery and get in depth the junction between tonsil and muscle. Sometimes difficult to identify in extreme lingual tonsil hyperplasia, foramen caecum is the key point for starting the dissection. This point must be stressed because it locates the upper limit of the resection, helping the surgeon to spare circumvallate papillae area and taste function, and in the same time giving to the surgeon a reasonable location of the midline. Approaching this step of the dissection with the scope tip relatively far from the surgical field (low magnification and a wide angle view of the surgical field) is strongly recommended in order to enhance the 3D awareness of the surgical anatomy. At the end of this first step lingual tonsil is completely split in midline, and a deep groove joining foramen caecum to midline glosso-epiglottic area at the lymphoid-muscle junction in depth is our goal.
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
