Fig. 1
Anatomic borders of the parapharyngeal space (area outlined by dots). Di Digastric muscle, Mas Masseter muscle, Mpt Medial pterygoid muscle, P Parotid gland, Scm Sternocleidomastoid muscle, Spc, Superior constrictor muscle (Courtesy of the Mayo Foundation, Rochester, Minn. Copy Right obtained from Mosby Elsevier)
Epidemiology
Parapharyngeal space tumors account for 0.5 % of all head and neck neoplasms. The majority (>80 %) of these PPS tumors are benign and a minority (<20 %) are malignant [1, 3]. See Table 1 for a more inclusive list. A recent systematic review of the literature on parapharyngeal space tumors by Riffat et al. reiterated this occurrence. The study found the most common primary PPS tumor originates in the salivary gland (45 %) and is found in the pre-styloid area [1, 3]. Pleomorphic adenomas were the most common benign salivary gland tumors (64 %) in the PPS [1, 3]. The second most common PPS tumors were found to be the neurogenic tumors (41 %) located mainly in the post-styloid area [1, 3]. The most common benign neurogenic tumor of the PPS was paragangliomas (52 %) followed by schwannomas (27 %) and neurofibromas (9 %). Prior studies reported schwannomas to be the most common neurogenic tumor [8]. The most common paragangliomas of the PPS were Vagus nerve in origin followed by carotid body tumors and glomus jugulare tumors [1].
Table 1
Parapharyngeal tumors
Origin | Benign | Malignant |
|---|---|---|
Salivary | Pleomorphic adenoma Warthins tumor Oncocytoma Lymphoepithelial cyst | Carcinoma ex-pleomorphic adenoma Adenoid cystic carcinoma Mucoepidermoid carcinoma Adenocarcinoma Acinic cell carcinoma |
Neurogenic | Carotid body tumor Vagal paraganglioma Neurofibroma Neurilemoma | Neurofibrosarcoma |
Lymphovascular | Hemangioma Hemangioepithelioma Venous malformation Lymphatic malformation | Lymphoma Hemangiopericytoma Plasmacytoma |
Metastatic | Thyroid Carcinoma Squamous Cell Carcinoma | |
Other | Lipoma Rhabdomyoma Leiomyoma Branchial cleft cyst Teratoma Meningioma Carotid artery aneurysm | Liposarcoma Rhabdomyosarcoma Chondrosarcoma Fibrosarcoma |
Less than 20 % of the PPS tumors were malignant [1, 3]. Out of all the salivary gland tumors in the PPS, 23 % were malignant. Adenoid cystic carcinomas (7 %) and mucoepidermoid carcinomas (4 %) were the most common malignant salivary gland neoplasms. Out of all the neurogenic tumors, 5 % were malignant. Metastatic disease is a rare occurrence in the PPS. Only 3 % of the tumors in the PPS were metastatic lesions [1]. However, this could be the result of incomplete data collection and reporting. Thyroid carcinoma is the most common metastatic lesion (20 %) of all the PPS cancers [1].
Clinical Presentation and Workup
It is more common for a clinician to encounter an asymptomatic patient presenting to the clinic with an incidentally found mass during a physical examination or on imaging that was performed as part of another workup. Approximately 50 % of patients are asymptomatic at presentation [9]. The most common sign (50 %) is intraoral swelling (Fig. 2), followed by a cervical mass (44 %) [1]. The PPS tumor is usually at least 2.5 cm before it is palpable as a cervical mass. When a post-styloid mass enlarges, it can compress the surrounding tissue, especially cranial nerves IX, X, XI, and XII. Cranial nerve neuropathy was reported as the third most common sign (18 %) behind neck mass and intraoral swelling [1]. The Vagus nerve was most commonly affected and was seen in 7 % of cases [1]. Medial enlargement of the mass combined with cranial nerve deficit produced dysphagia (11 %) and dysphonia (9 %) [1]. Although clinically interesting, Horner syndrome, known by the triad of ptosis, miosis, and anhydrosis of the ipsilareral face, was seen in only 2 % of cases [1]. Hearing loss and middle ear effusion are seen when superior enlargement of the mass causes Eustachian tube compression.

Fig. 2
Right oropharyngeal mass at presentation. Arrow points to displaced uvula
Imaging
Cross sectional, anatomic imaging studies are of paramount importance in diagnosing and developing treatment plans for patients with PPS tumors. The complex anatomic location prevents complete assessment of any PPS mass with physical examination and endoscopy alone. Computed tomography (CT) scan with contrast and magnetic resonance imaging (MRI) with gadolinium are the most widely used imaging modalities for PPS tumors. CT and MRI scans are complimentary in the evaluation since CT scans can provide better bony details such as skull base erosion and MRI scans provide better soft tissue detail without the need for ionizing radiation (Fig. 3) [3, 10]. Given that the majority of the PPS tumors are of salivary or neurogenic origin, MRI with gadolinium is the preferred imaging tool. Besides providing the size, shape, extent of disease, and adjacent structures, it also provides the location (pre- and post-styloid) based on the displacement of the parapharyngeal fat, internal carotid artery and internal jugular vein (Table 2) [10]. However, PPS fat can be less discerning with increasing tumor size. CT and MRI scans can indicate malignancy in the presence of irregular tumor margins and invasion into the surrounding tissue plane. Schwannomas and paragangliomas have specific imaging and enhancing characteristics such as “salt and pepper” appearance on MRI for paragangliomas. In addition, CT and MR angiography can be valuable in assessing vascularity of the tumor and/or vascular invasion by the tumor.
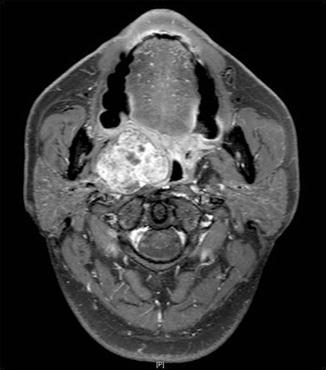
Fig. 3
Magnetic resonance image: right PPS pleomorphic adenoma
Table 2
Image findings in pre and post-styloid contents
PPS Location | Image findings |
|---|---|
Pre-styloid | 1. Mass in the anterior PPS, displacing the PPS fat medially and posteriorly 2. Displacement of the posterior belly of the digastric and styloid muscle group posteriorly 3. Location medial to and separable from the medial pterygoid muscle 4. Mass is anterior to the ICA and IJV |
Post-styloid | 1. Mass in the posterior or medial PPS 2. Extension posterior to the styloid process rather than anteriorly via the stylomandibular tunnel 3. Lateral and anterior displacement of the posterior belly of the digastric and styloid muscle group 4. Anterior displacement of the ICA and IJV |
Diagnosis
Having a tissue diagnosis is invaluable in making treatment decisions. It will also help with obtaining consent from the patient for surgery, discussing morbidity, cure rate, and recurrence. Fine needle aspiration (FNA) Biopsy of the PPS mass has mixed published results. It is, however, the least morbid or invasive way to obtain a diagnosis when feasible. In our institution, when an Ultrasound guided FNA is not possible due to the tumor location, CT guided FNA has been successful in obtaining a diagnosis. Open biopsy, whether it is transoral or transcervical, has been universally discouraged [11, 12]
Treatment
The primary treatment modality for PPS tumors is surgery [1, 3]. Over the decades, several surgical approaches to PPS tumors have been developed. In the most recent systematic review of the past 20 years of literature on PPS tumors, the transcervical approach was the most commonly used (48 %) followed by cervical-parotid approach (27 %), cervical approach with mandibulotomy (9 %), and the transoral approach (2 %) [1]. The best and safest approach is chosen after careful deliberation of tumor size, pathology, location within the PPS along with the best surgical access.
The PPS tumors located in the inferior aspect can be approached via the cervical approach. It provides the best direct access with good visualization of the cranial nerves and the great vessels. PPS tumors located in the middle and upper aspect with facial nerve involvement can be accessed via the cervical-parotid approach (Fig. 4) [7]. This approach allows access to the deep lobe of the parotid and the great vessels [3, 6, 11]. Large tumors located in the upper PPS can be accessed via the cervical approach with a median or a paramedian mandibulotomy (Fig. 5) [3, 6, 7, 11].
Fig. 4
Cervical-parotid approach
Fig. 5
Cervical-parotid approach with midline mandibulotomy
In order to overcome some of the disadvantages of the open surgery, Duvvuri et al recently described a novel transcervical, minimally invasive, video assisted, image guided technique [13]. It facilitated resection of the PPS mass using bony landmarks for guidance in four patients with good outcomes and showed its feasibility [13]. However, long-term follow-up in a larger cohort is needed.
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


