Purpose
To estimate the long-term cumulative risk of late posterior chamber intraocular lens (IOL) dislocation after cataract extraction in a population-based cohort.
Design
Retrospective cohort study and nested case-control study.
Methods
The records of all residents of Olmsted County, Minnesota, who underwent cataract extraction from January 1, 1980, through May 31, 2009, (14 471 cases in 9577 residents) and who were diagnosed with late posterior chamber IOL dislocation in the same period were reviewed. Cases were identified through the Rochester Epidemiology Project. Three controls chosen from the cataract surgery cohort were matched to each IOL dislocation case by age, gender, and duration of follow-up. Records were reviewed to confirm case status and to ascertain risk factor information. The cumulative risk of IOL dislocation was estimated by using the Kaplan-Meier method. Logistic regression models assessed differences between cases and controls.
Results
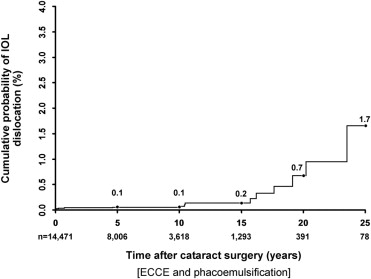
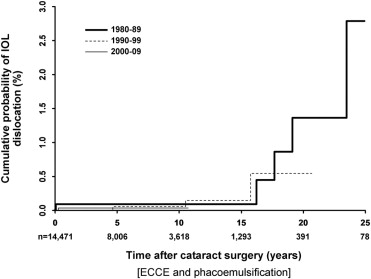
We identified 16 cases of late posterior chamber IOL dislocation, 9 with in-the-bag dislocations and 7 with out-of-the-bag dislocations. At 5, 10, 15, 20, and 25 years after cataract extraction, the cumulative risk of IOL dislocation was 0.1%, 0.1%, 0.2%, 0.7%, and 1.7%, respectively. There was no significant difference in the risk of late IOL dislocation after extracapsular cataract extraction when compared with phacoemulsification ( P = .21) or between different decades of surgery ( P = .92). Pseudoexfoliation and zonular laxity at surgery were associated significantly with late IOL dislocation ( P = .01).
Conclusions
The long-term cumulative risk of late IOL dislocation after cataract extraction was low and did not significantly change over our nearly 30-year study period.
Posterior chamber intraocular lens (IOL) dislocation as a late complication of cataract extraction has been reported with increasing frequency in recent years, leading to concerns of a pending large increase in IOL dislocations needing surgical intervention. A dislocated IOL often requires explantation or repositioning with subsequent serious potential complications, such as retinal tear, retinal detachment, and vitreous hemorrhage.
It is not known if the observed increased number of late IOL dislocations is the result of an increased rate of incidence of IOL dislocations or simply a larger community of at-risk pseudophakic patients. Recently, 2 population-based studies in Sweden estimated that the incidence of late IOL dislocation is low after phacoemulsification, but the authors were unable to demonstrate significantly an increased rate of incidence. Similar population-based studies in the United States are not available.
The purpose of our population-based cohort study was to report the cumulative probability and the risk factors of late posterior chamber IOL dislocation after phacoemulsification and extracapsular cataract extraction (ECCE) in the stable, well-defined population of Olmsted County, Minnesota, during the nearly 30-year period from 1980 through 2009.
Methods
Data Source
Data were obtained by using the resources of the Rochester Epidemiology Project, a medical record linkage system established in 1966 to facilitate performance of population-based studies among residents of Rochester and surrounding Olmsted County, Minnesota. Virtually all medical care for this relatively isolated semiurban county (2000 total county population, 124 277) is provided by the Mayo Clinic, Olmsted Medical Group, and their affiliated hospitals. The Rochester Epidemiology Project links the Mayo Clinic’s medical record system with the Olmsted Medical Group as well as other potential providers of medical care, including the University of Minnesota and Department of Veterans Affairs hospitals in Minneapolis 90 miles north of Rochester, other hospitals in surrounding counties, and the few independent medical practices in Olmsted County. Consequently, the Rochester Epidemiology Project provides a medical records linkage and retrieval system for virtually all sources of medical care used by the Olmsted County population. The usefulness and accuracy of the Rochester Epidemiology Project electronic databases for population-based studies of disease cause and outcomes have been well established.
Rochester Epidemiology Project Cataract Surgery Cohort
Incident cases of cataract extraction performed on all Olmsted County residents between January 1, 1980, and May 31, 2009, were identified by using previously published and updated resources of the Rochester Epidemiology Project. The Rochester Epidemiology Project cataract surgery cohort included 14 471 surgeries performed on 9577 Olmsted County residents of all ages and represented a predominantly white (96%) population. Cataract extraction performed by using phacoemulsification or ECCE as a primary procedure or a combined procedure with penetrating keratoplasty or trabeculectomy was included. Intracapsular cataract extraction, lensectomy combined with a planned pars plana vitrectomy, or cataract surgery in the surgical management of ocular trauma were excluded. Reliability tests on the data were performed and verified the accuracy of coded demographic and clinical data and estimated case over ascertainment of this cohort at < 1%.
Rochester Epidemiology Project Intraocular Lens Dislocation Cohort
We used Mayo Clinic modifications of International Classification of Diseases, Ninth Edition 9, Clinical Modification, diagnosis codes 379.32, 379.33, 379.34, 379.39, and 379.53 and International Classification of Diseases, Ninth Edition 9, Clinical Modification procedure codes 13.8 and 13.72 retrospectively to identify all potential IOL dislocation-related diagnoses made or procedures performed on residents in the Rochester Epidemiology Project cataract surgery cohort. Late IOL dislocation was defined as any posterior chamber IOL requiring IOL repositioning or exchange surgery that occurred more than 90 days after the primary cataract surgery in which the initial postoperative IOL position was noted as good in the operative report. We excluded early IOL dislocations that occurred at the time of surgery or in the immediate 90-day postoperative period. The medical records of all identified patients were reviewed to ensure the accuracy of the demographic and clinical data, that cataract surgery and IOL dislocation were matched to the same eye, and to verify residence by using previously validated procedures.
In the nested case-control study, we compared each incident case with approximately 3 control cases from the Rochester Epidemiology Project cataract surgery cohort who did not have an IOL dislocation. Controls were matched to cases by age, gender, and length of follow-up.
Data Collection and Analysis
The records of all identified cohort and control cases were reviewed for data obtained before cataract surgery, including gender, date of birth, presence of pseudoexfoliation, glaucoma, macular degeneration, retina disease or surgery, uveitis, degree of myopia, axial length, keratometry, and trauma. Intraoperative data included date and technique of cataract surgery, IOL optic material, location of incision, anterior capsulotomy technique, capsular rupture, use of mechanical pupil dilation, or capsular tension ring. Data collected on IOL dislocation cases included type of IOL dislocation (in-the-bag vs out-of-the-bag), date of dislocation, surgical management, and vision before and after surgical repositioning or exchange.
The cumulative risk of IOL dislocation after cataract surgery was estimated by using the Kaplan-Meier method. The duration of follow-up care after cataract surgery was based on the resident’s last computer documented reregistration date for any medical care within the REP or documented death. Differences between cases and controls were evaluated by using conditional logistic regression analysis. The Fisher exact test was used for comparisons with small numbers.
Results
Medical record review identified 32 potential cases with a documented IOL dislocation after cataract surgery. Exclusion of 13 nonresidents and 3 anterior chamber IOL dislocations left 16 incident cases of late posterior chamber IOL dislocation in 16 residents. Table 1 shows the demographics and clinical data for the cataract surgery and IOL dislocation cohorts. Seven (44%) of the 16 IOL dislocations were out-of-the-bag cases in which the IOL migrated through a defect in the posterior capsule or zonule. Nine (56%) were in-the-bag cases in which the IOL remained within the capsular bag and the entire IOL–bag complex dislocated. All IOL dislocations were in white residents. Fourteen (88%) of the 16 cases were managed by IOL exchange and 2 (12%) were repositioned by using scleral fixation sutures. The median preoperative Snellen visual acuity was 20/150 (25% to 75% quartile, 20/60 to 20/250), and the median Snellen visual acuity after repositioning or exchange was 20/50 (25% to 75% quartile, 20/25 to 20/150), with 43% of eyes reaching a Snellen visual acuity of 20/40 or better.
| Variable | Primary Cataract Surgery Cohort, n (%) | IOL Dislocation Cohort, n (%) |
|---|---|---|
| Gender | ||
| Male | 5360 (37) | 8 (50) |
| Female | 9111 (63) | 8 (50) |
| Cataract surgery technique | ||
| Phacoemulsification | 10 563 (73) | 10 (62) |
| ECCE | 3589 (25) | 6 (38) |
| Other | 319 (2) | 0 (0) |
| Decade of surgery | ||
| 1980 through 1989 | 2241 (15) | 6 (38) |
| 1990 through 1999 | 4624 (32) | 6 (38) |
| 2000 through 2009 | 7606 (53) | 4 (24) |
| Age (y) | ||
| 0 to 9 | 27 (0.2) | 0 (0) |
| 10 to 19 | 24 (0.2) | 0 (0) |
| 20 to 29 | 38 (0.3) | 0 (0) |
| 30 to 39 | 91 (0.6) | 0 (0) |
| 40 to 49 | 396 (2.7) | 0 (0) |
| 50 to 59 | 1084 (7.5) | 2 (13) |
| 60 to 69 | 2823 (19.5) | 8 (50) |
| 70 to 79 | 5479 (37.9) | 5 (31) |
| 80 to 89 | 3997 (27.6) | 1 (6) |
| ≥ 90 | 512 (3.5) | 0 (0) |
| Total | 14 471 (100) | 16 (100) |
The cumulative risk of IOL dislocation up to 25 years after cataract surgery is shown in Figure 1 . The mean interval between cataract surgery and IOL dislocation was 6.2 ± 7.7 years in the out-of-the-bag group compared with 12.4 ± 8.2 years in the in-the-bag group ( P = .14). There was no significant difference in late IOL dislocation rates when comparing cataract surgery performed in the 1980s (0.1%), 1990s (0.1%), and 2000s (0.1%) and followed to 10 years ( P = .92; Figure 2 ). Our study had 90% power to detect at least a 0.5% difference in IOL dislocation rates between any of the 2 decade groups.
In the case-control portion of the study, 16 cases (8 men, 8 women) with IOL dislocation after cataract surgery were matched by age, gender, date of surgery, and length of follow-up with 47 controls (24 men, 23 women). The mean age at cataract extraction was 69 ± 9 years in cases and 70 ± 10 years in controls. Before surgery, the degree of myopia trended higher in IOL dislocation cases (−1.80 ± 3 diopters [D]) than in controls (−0.40 ± 2.0 D), but the difference was not significant ( P = .07). We found no association between IOL dislocation and axial length in cases (23.89 ± 1.28 mm) versus controls (23.84 ± 1.21 mm; P = .51) and in keratometry in cases (43.74 ± 1.65 D) versus controls (43.53 ± 1.47 D; P = .83). Univariate associations between other selected variables and IOL dislocation are shown in Table 2 .
| Variable | Cases, n (%) | Controls, n (%) | P Value |
|---|---|---|---|
| Preoperative | |||
| Pseudoexfoliation | |||
| Yes | 3 (19) | 0 (0) | |
| No | 13 (81) | 47 (100) | .01 a |
| Open-angle glaucoma | |||
| Yes | 3 (19) | 2 (4) | |
| No | 13 (81) | 45 (96) | .09 b |
| Previous anterior vitrectomy | |||
| Yes | 0 (0) | 2 (4) | |
| No | 16 (100) | 45 (96) | 1.0 a |
| Age-related macular degeneration | |||
| Yes | 3 (19) | 8 (17) | |
| No | 13 (81) | 39 (83) | .84 b |
| Uveitis | |||
| Yes | 1 (6) | 0 (0) | |
| No | 15 (94) | 47 (100) | .25 a |
| Previous trauma | |||
| Yes | 1 (6) | 1 (2) | |
| No | 15 (94) | 46 (98) | .44 b |
| Intraoperative | |||
| Zonular dehiscence or laxity | |||
| Yes | 3 (19) | 0 (0) | |
| No | 13 (81) | 47 (100) | .01 a |
| Surgical technique | |||
| Phacoemulsification | 10 (63) | 26 (55) | |
| ECCE | 6 (37) | 21 (45) | .24 b |
| IOL optic material | |||
| Acrylic | 3 (19) | 16 (34) | |
| Silicone | 3 (19) | 5 (11) | |
| Polymethylmethacrylate | 10 (62) | 26 (55) | .45 b |
| Incision | |||
| Temporal clear cornea | 4 (25) | 19 (40) | |
| Superior scleral tunnel | 12 (75) | 28 (60) | .12 b |
| Anterior capsulotomy | |||
| CCC | 11 (69) | 26 (55) | |
| Can opener | 5 (31) | 21 (45) | .12 b |
| Capsule rupture | |||
| Yes | 0 (0) | 1 (2) | |
| No | 16 (100) | 46 (98) | 1.0 a |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


