Purpose
To evaluate the risk, risk factors, and visual impact of choroidal neovascularization (CNV) in uveitis cases.
Design
Retrospective cohort study.
Methods
Standardized medical record review at 5 tertiary centers.
Results
Among 15 137 uveitic eyes (8868 patients), CNV was rare in the cases of anterior or intermediate uveitis. Among the 4041 eyes (2307 patients) with posterior uveitis or panuveitis, 81 (2.0%) had CNV at presentation. Risk factors included posterior uveitis in general and specific uveitis syndromes affecting the outer retina–retinal pigment epithelium–choroid interface. Among the 2364 eyes (1357 patients) with posterior uveitis or panuveitis and free of CNV at the time of cohort entry, the cumulative 2-year incidence of CNV was 2.7% (95% confidence interval [CI], 1.8% to 3.5%). Risk factors for incident CNV included currently active inflammation (adjusted hazard ratio [aHR], 2.13; 95% CI, 1.26 to 3.60), preretinal neovascularization (aHR, 3.19; 95% CI, 1.30 to 7.80), and prior diagnosis of CNV in the contralateral eye (aHR, 5.79; 95% CI, 2.77 to 12.09). Among specific syndromes, the incidence was greater in Vogt-Koyanagi-Harada syndrome (aHR, 3.37; 95% CI, 1.52 to 7.46) and punctate inner choroiditis (aHR, 8.67; 95% CI, 2.83 to 26.54). Incident CNV was associated with a 2-line loss of visual acuity (+0.19 logarithm of the minimal angle of resolution units; 95% CI, 0.079 to 0.29) from the preceding visit.
Conclusions
CNV is an uncommon complication of uveitis associated with visual impairment that occurs more commonly in forms affecting the outer retina–retinal pigment epithelium–choroid interface, during periods of inflammatory activity, in association with preretinal neovascularization, and in second eyes of patients with unilateral CNV. Because CNV is treatable, a systematic approach to early detection in high-risk patients may be appropriate.
Choroidal neovascularization (CNV) consists of pathologic blood vessel growth from the choroid across Bruch’s membrane into the retina. The pathogenesis of choroidal neovascularization involves a disruption of the homeostasis between the retinal pigment epithelium (RPE) and Bruch’s membrane. The proliferating choroidal blood vessels then extend into the subretinal space, often in the region of the macula, where they can leak fluid and lead to serous retinal detachment and scarring, often resulting in central vision loss. CNV can arise as a complication of virtually any pathogenic process that involves the RPE and damages Bruch’s membrane.
Although CNV is most well known as being associated with age-related macular degeneration (AMD), it also can be a severe sight-threatening complication resulting from both infectious and noninfectious uveitis. As an important cause of vision loss among people younger than 50 years, CNV not infrequently strikes patients during some of their most highly productive years, particularly in the setting of uveitis, which also tends to affect a working-age population. If left untreated, CNV is associated with a poor prognosis. Fortunately, recent advances in the treatment of CNV allow for the possibility of improved visual outcomes, particularly in cases detected at an early stage.
Because of the association between CNV and uveitis and the potential for severe vision loss resulting from CNV, better characterization of the risk of and risk factors for CNV in this population is needed. We evaluated these issues in a large, retrospective, multicenter cohort study of uveitis cases.
Methods
Institutional review board approval for the Systemic Immunosuppressive Therapy for Eye Diseases (SITE) cohort study was obtained and maintained at each center’s governing institutional review board before and throughout the period of data collection. Each institution’s institutional review board approved a waiver of consent and Health Insurance Portability and Accountability Act exemption for this study because it entailed retrospective chart review. The project was conducted in adherence with the principles of the Declaration of Helsinki and all federal and state laws in the United States. The methods of the SITE cohort study previously have been described in detail.
This was a retrospective cohort study of patients with noninfectious ocular inflammatory diseases seen between 1978 and 2007 at 5 academic ocular inflammation centers in the United States. Patients with known HIV infection were excluded. Some previous SITE reports described using a random sample of approximately 40% of the eligible patients at 1 of the centers plus all eligible patients at the other 4 centers. However, by the time of this analysis, data regarding all eligible patients with available charts at all 5 centers were available and were used for this analysis.
A protocol-driven structured chart review was conducted for each patient studied, with data entered into a standardized form in a computerized database customized for the SITE cohort study. Data collection procedures included several quality assurance techniques and extensive cross-checks, allowing correction of likely errors in real time, in addition to monitoring of data entry quality through site visiting. For this analysis, only the cases of uveitis were studied. Data used included demographic characteristics, ocular inflammatory diagnoses, and ophthalmologic examination findings, such as visual acuity and inflammatory disease activity.
Ascertainment of Outcomes
Outcomes assessed included the presence of CNV at cohort entry, the incidence of CNV during follow-up, the incidence of CNV in second eyes of patients with initially unilateral CNV, and changes in visual acuity in relation to CNV. CNV was diagnosed based on chart notes; either a clinically definite diagnosis or a diagnosis based on ancillary testing was accepted as representing CNV. The database did not discriminate between cases with active CNV and those with evidence of prior CNV (eg, classic disciform scar).
The incidence of CNV was calculated by observing the eyes without CNV at the time of cohort entry until the first notation of CNV, up to the time that the patient ceased attending the clinic or the study completion at the patient’s site. Potential risk factors for CNV evaluated included demographic characteristics, ocular inflammatory diagnoses, and ophthalmologic examination findings. These ophthalmologic examination findings included visual acuity, time-updated inflammatory disease activity (classified as active, slightly active [reflecting minimal activity designated by descriptors such as “trace”], or inactive), and the presence and extent of anterior chamber cells, vitreous cells, and vitreous haze. Anterior chamber cells and vitreous haze were recorded using an ordinal scale in a manner as similar as possible in a retrospective study to standards promoted by an expert consensus group ; vitreous cells can be viewed as an ordinal grading.
Statistical Analysis
To evaluate risk factors associated with prevalent CNV at cohort entry, crude and adjusted odds ratios were calculated using univariate and multivariate logistic regression that incorporated generalizations of generalized estimating equations to account for correlation between the eyes of individual patients. Potential risk factors for incidence of CNV were evaluated on the basis of hazard ratios (HRs) and adjusted HRs (with 95% confidence intervals [CIs]), which were generated using crude and multivariate Cox proportional hazards models with a robust sandwich estimate to account for correlation between the eyes of individual patients. Incidence of CNV at 2 years (the median follow-up time) was evaluated by calculating the cumulative incidence estimated from the crude Cox regression hazard function, which allowed incidence estimates consistent with the hazard ratios for time-varying risk factors as well as 95% CIs accounting for correlation between eyes of the same patient. The risk of CNV developing in the second eye was evaluated by including the presence of CNV in the contralateral eye as a time-updated covariate in the incidence analysis and separately by Kaplan-Meier analysis of contralateral-eye CNV incidence among patients with bilateral uveitis and unilateral CNV in the cohort. To determine the visual acuity change associated with the development of CNV, the logarithm of the minimal angle of resolution equivalent visual acuity at the visit before CNV diagnosis was compared with that at the time of CNV diagnosis using a t test. All statistical analyses were performed with SAS software version 9.3 (SAS Institute, Cary, North Carolina, USA).
Results
Among 15 137 eyes with uveitis (8868 patients) in the SITE cohort, an initial evaluation of the prevalence of CNV by the site of inflammation demonstrated that CNV was very rare in cases of anterior or intermediate uveitis: only 4 eyes (0.06%; 3 patients [0.07%]) with anterior uveitis had CNV at presentation, and there were no patients with intermediate uveitis who had CNV at presentation. Among eyes seen more than once, there were 15 cases among 4103 eyes with anterior uveitis (2542 patients) seen over a mean of 2.8 years, yielding a 0.13% CNV/eye-year incidence rate. There were 7 cases among 1982 eyes with intermediate uveitis (1085 patients) seen over a mean of 3.2 years, yielding a 0.11% CNV/eye-year incidence rate. Given that the very small number of prevalent and incident CNV events among intermediate and anterior uveitis cases provided little information on which to do a risk factor analysis, we limited the remainder of the analysis to cases of posterior uveitis or panuveitis.
Among cases of posterior uveitis or panuveitis, data were available for 4041 eyes of 2307 patients. The median age was 38 years (range, 0 to 89 years). The study population was predominantly female (64%) and white (70%). Most patients (90%) had bilateral uveitis at presentation.
Prevalence of Choroidal Neovascularization
At the time of initial presentation, 81 eyes with posterior uveitis or panuveitis were found to have active CNV or sequelae of past CNV, yielding an overall prevalence of 2.0% (95% CI, 1.6% to 2.4%) among cases of posterior uveitis or panuveitis seeking tertiary uveitis care. Patients with CNV were not significantly different than those without CNV in terms of age, sex, or race ( Table 1 ). The prevalence of CNV was significantly lower among eyes of current smokers (0.9%) and somewhat lower among past smokers (2.1%) when compared with those who had never smoked (2.6%; overall P = .02).
| Characteristic | No. of Eyes | No. of Eyes with Choroidal Neovascularization | Prevalence (%) | Crude Odds Ratio (95% Confidence Interval) | Crude P Value | Adjusted Odds Ratio a (95% Confidence Interval) | Overall Adjusted P Value |
|---|---|---|---|---|---|---|---|
| Age at uveitis diagnosis (y) | .81 | .43 | |||||
| ≤35 | 1784 | 38 | 2.1 | Reference | Reference | ||
| >35 | 2255 | 43 | 1.9 | 0.94 (0.56 to 1.57) | 0.81 (0.48 to 1.35) | ||
| Gender | .57 | .81 | |||||
| Male | 1437 | 26 | 1.8 | Reference | Reference | ||
| Female | 2604 | 55 | 2.1 | 1.17 (0.68 to 2.02) | 1.07 (0.62 to 1.87) | ||
| Race | .05 | .25 | |||||
| White | 2833 | 62 | 2.2 | Reference | Reference | ||
| Black | 534 | 9 | 1.7 | 0.76 (0.35 to 1.67) | 1.18 (0.54 to 2.56) | ||
| Hispanic | 251 | 7 | 2.8 | 1.33 (0.54 to 3.25) | 1.66 (0.69 to 4.00) | ||
| Other | 423 | 3 | 0.7 | 0.33 (0.10 to 1.10) | 0.48 (0.15 to 1.53) | ||
| Smoking | .02 | .03 | |||||
| Never | 2027 | 53 | 2.6 | Reference | Reference | ||
| Past | 528 | 11 | 2.1 | 0.74 (0.33 to 1.66) | 0.76 (0.34 to 1.71) | ||
| Current | 778 | 7 | 0.9 | 0.35 (0.14 to 0.84) | 0.34 (0.14 to 0.83) | ||
| Unknown | 708 | 10 | 1.4 | 0.51 (0.24 to 1.08) | 0.62 (0.29 to 1.33) | ||
| Uveitis category | <.01 | <.01 | |||||
| Posterior uveitis | 2512 | 69 | 2.7 | Reference | Reference | ||
| Panuveitis | 1529 | 12 | 0.8 | 0.29 (0.15 to 0.56) | 0.26 (0.14 to 0.51) | ||
| Posterior/panuveitis subtype b | <.01 | <.01 | |||||
| Undifferentiated panuveitis | 1159 | 11 | 0.9 | Reference | Reference | ||
| Multifocal choroiditis with panuveitis | 615 | 28 | 4.6 | 4.55 (2.04 to 10.14) | 4.27 (1.94 to 9.39) | ||
| Multiple evanescent white dot syndrome | 21 | 3 | 14.3 | 18.58 (4.60 to 75.11) | 26.98 (6.25 to 116.40) | ||
| Birdshot retinochoroiditis | 397 | 4 | 1.0 | 0.99 (0.31 to 3.19) | 1.19 (0.34 to 4.18) | ||
| Vogt-Koyanagi-Harada syndrome | 320 | 1 | 0.3 | 0.30 (0.04 to 2.35) | 0.22 (0.03 to 1.73) | ||
| Retinal vasculitis | 727 | 6 | 0.8 | 0.78 (0.23 to 2.63) | 0.95 (0.28 to 3.15) | ||
| Punctate inner choroiditis | 17 | 2 | 11.8 | 15.03 (5.05 to 44.79) | 15.90 (5.11 to 49.43) | ||
| Serpiginous choroiditis | 148 | 7 | 4.7 | 5.27 (1.82 to 15.25) | 5.69 (1.93 to 16.82) | ||
| Other c | 637 | 19 | 3.0 | 2.39 (0.98 to 5.80) | 2.43 (1.02 to 5.81) | ||
| Bilateral uveitis | .12 | .15 | |||||
| No | 389 | 13 | 3.3 | Reference | Reference | ||
| Yes | 3652 | 68 | 1.9 | 0.55 (0.29 to 1.03) | 0.58 (0.31 to 1.09) | ||
| Visual acuity | <.01 | <.01 | |||||
| 20/40 or better | 1695 | 17 | 1.0 | Reference | Reference | ||
| >20/40 to <20/200 | 1429 | 35 | 2.4 | 3.25 (1.60 to 6.60) | 3.24 (1.69 to 6.23) | ||
| 20/200 or worse | 907 | 29 | 3.2 | 3.88 (1.87 to 8.05) | 4.06 (2.06 to 7.99) | ||
| Missing | 10 | 0 | 0.0 | n/a | n/a |
a Adjusted by race, smoking, uveitis category, and visual acuity.
b Posterior uveitis/panuveitis subtype was not adjusted by uveitis category because they are different ways of considering the same variable.
c Includes several conditions too infrequent to analyze separately: sympathetic ophthalmia, acute posterior multifocal placoid pigment epitheliopathy, neuroretinitis, diffuse retinochoroiditis, focal retinochoroiditis, acute retinal necrosis syndrome, Eales disease, unspecified inflammatory chorioretinal scars, sarcoidosis, and necrotizing retinitis.
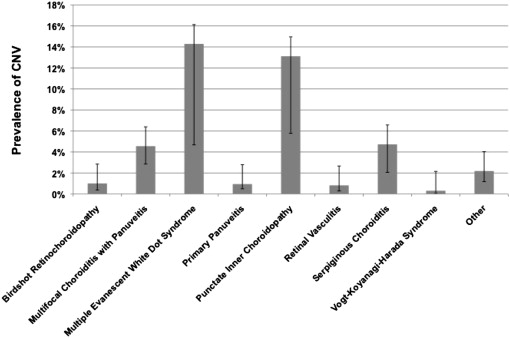
The anatomic site of inflammation was associated significantly with CNV at presentation, with panuveitis (0.8%) having a lower prevalence of CNV than posterior uveitis (2.7%; adjusted odds ratio [aOR], 0.26; 95% confidence interval [CI], 0.14 to 0.51). Compared with eyes with panuveitis that did not fit a specific morphologic syndrome (prevalence of CNV at 0.9%), eyes that had been diagnosed with certain posterior uveitis or panuveitis syndromes that affect the region of the choroid and RPE were more likely to have CNV at presentation (all P < .01), including multifocal choroiditis with panuveitis (4.6%; aOR, 4.27; 95% CI, 1.94 to 9.39), multiple evanescent white dot syndrome (14.3%; aOR, 26.98; 95% CI, 6.25 to 116), punctate inner choroiditis (11.8%; aOR, 15.90; 95% CI, 5.11 to 49.43), and serpiginous choroiditis (4.7%; aOR, 5.69; 95% CI, 1.93 to 16.82; see also Figure 1 ). Because CNV often occurred well before presentation, we did not evaluate the inflammatory status at the time of presentation as a risk factor for prevalent CNV.
Worse visual acuity was more common among eyes with CNV at presentation, which had more than 4 times higher odds of a visual acuity of 20/200 or worse with respect to 20/40 or better than eyes without CNV at presentation (aOR, 4.06; 95% CI, 2.06 to 7.99; P < .001).
Incidence of Choroidal Neovascularization and Risk Factors for Developing Choroidal Neovascularization
At the time of cohort entry, 2364 eyes of 1357 patients had posterior uveitis or panuveitis and were free of CNV for which 1 or more follow-up visits were available. These were followed up for incidence of CNV over a median of 1.98 years (interquartile range, 0.48 to 5.24 years). The overall cumulative incidence of CNV by the 2-year time point was estimated to be 2.7% (95% CI, 1.8% to 3.5%; Figure 2 ). Inspection of the Kaplan-Meier curve indicates that the risk was considerably higher over the first 6 months after presentation, reaching nearly 2% by that point, and then increased less rapidly over time thereafter.
Several risk factors for incident CNV were identified (see Table 2 ). In contrast to the results of the prevalence analysis, there was no significant difference in the 2-year incidence of CNV between eyes with posterior uveitis (2.9%) and eyes with undifferentiated panuveitis (2.5%; adjusted hazard ratio [aHR], 0.87; 95% CI, 0.54 to 1.41). Compared with eyes with panuveitis that did not fit another morphologic syndrome (which had an estimated 2-year incidence of CNV of 1.5%), Vogt-Koyanagi-Harada disease (6.4%; aHR, 3.37; 95% CI, 1.52 to 7.46), and punctate inner choroiditis (13.2%; aHR, 8.67; 95% CI, 2.83 to 26.54) were associated with increased CNV risk. Multifocal choroiditis with panuveitis also tended to have an increased risk (3.6%; aHR, 2.19; 95% CI, 1.01 to 4.78), whereas no statistically significant increase in incidence with serpiginous retinochoroiditis was observed (2.7%; aHR, 1.56; 95% CI, 0.51 to 4.77). Too few cases of multiple evanescent white dot syndrome were available for incidence analysis to evaluate CNV risk for that syndrome.
| Characteristic | No. of Eyes at Risk | 2-Year Incidence of CNV (95% Cl) | Crude Hazard Ratio (95% CI) | Crude P Value | Adjusted Hazard Ratio a (95% CI) | Overall Adjusted P Value |
|---|---|---|---|---|---|---|
| Overall cases | 2364 | 2.7% (1.8% to 3.5%) | n/a | n/a | n/a | n/a |
| Age at uveitis diagnosis (y) | .62 | .28 | ||||
| ≤35 | 1066 | 2.5% (1.5% to 3.5%) | Reference | Reference | ||
| >35 | 1298 | 2.8% (1.7% to 4.0%) | 1.13 (0.69 to 1.86) | 1.32 (0.80 to 2.17) | ||
| Gender | .61 | .19 | ||||
| Male | 826 | 2.9% (1.6% to 4.2%) | Reference | Reference | ||
| Female | 1538 | 2.6% (1.6% to 3.5%) | 0.88 (0.53 to 1.45) | 0.72 (0.44 to 1.17) | ||
| Race | .08 | .17 | ||||
| White | 1617 | 2.3% (1.3% to 3.2%) | Reference | Reference | ||
| Black | 380 | 3.6% (1.7% to 5.5%) | 1.61 (0.90 to 2.89) | 1.59 (0.89 to 2.84) | ||
| Hispanic | 166 | 5.4% (1.7% to 9.1%) | 2.46 (1.13 to 5.34) | 2.02 (0.93 to 4.39) | ||
| Other | 201 | 2.3% (0.3% to 4.2%) | 1.02 (0.40 to 2.57) | 0.95 (0.35 to 2.55) | ||
| Smoking | .74 | .88 | ||||
| Never | 1206 | 2.6% (1.6% to 3.5%) | Reference | Reference | ||
| Past | 301 | 3.0% (1.1% to 4.9%) | 1.18 (0.60 to 2.31) | 1.22 (0.62 to 2.42) | ||
| Current | 499 | 2.2% (0.8% to 3.7%) | 0.86 (0.42 to 1.75) | 0.95 (0.47 to 1.93) | ||
| Unknown | 358 | 3.4% (1.2% to 5.6%) | 1.34 (0.67 to 2.67) | 1.24 (0.62 to 2.46) | ||
| Uveitis category b | .56 | .57 | ||||
| Posterior uveitis | 1399 | 2.9% (1.8% to 3.9%) | Reference | Reference | ||
| Panuveitis | 965 | 2.5% (1.4% to 3.5%) | 0.86 (0.52 to 1.43) | 0.87 (0.54 to 1.41) | ||
| Posterior uveitis/panuveitis subtype | <.01 | <.01 | ||||
| Undifferentiated panuveitis | 725 | 1.5% (0.6% to 2.3%) | Reference | Reference | ||
| Multifocal choroiditis with panuveitis | 350 | 3.6% (1.5% to 5.6%) | 2.47 (1.13 to 5.42) | 2.19 (1.01 to 4.78) | ||
| Multiple evanescent white dot syndrome | 9 | 0% | n/a | n/a | ||
| Birdshot retinochoroiditis | 261 | 2.6% (0.6% to 4.6%) | 1.79 (0.71 to 4.55) | 1.67 (0.65 to 4.29) | ||
| Vogt-Koyanagi-Harada syndrome | 209 | 6.4% (2.8% to 9.9%) | 4.50 (2.06 to 9.82) | 3.37 (1.52 to 7.46) | ||
| Retinal vasculitis | 429 | 1.8% (0.4% to 3.2%) | 1.23 (0.49 to 3.08) | 1.22 (0.47 to 3.17) | ||
| Punctate inner choroiditis | 12 | 10.1% (0.0% to 25.8%) | 9.64 (3.13 to 29.69) | 8.67 (2.83 to 26.54) | ||
| Serpiginous choroiditis | 76 | 2.7% (0.0% to 5.6%) | 1.85 (0.56 to 6.16) | 1.56 (0.51 to 4.77) | ||
| Other c | 293 | 3.2% (1.0% to 5.3%) | 1.51 (0.55 to 4.09) | 1.63 (0.60 to 4.42) | ||
| Preretinal neovascularization d | .04 | .01 | ||||
| No | 2.6% (1.7% to 3.4%) | Reference | Reference | |||
| Yes | 6.1% (1.2% to 10.8%) | 2.43 (1.04 to 5.69) | 3.19 (1.30 to 7.80) | |||
| Inflammatory activity d | .03 | .02 | ||||
| Inactive | 1.9% (1.0% to 2.7%) | Reference | Reference | |||
| Slightly active | 3.4% (1.3% to 5.6%) | 1.84 (0.91 to 3.74) | 1.85 (0.90 to 3.81) | |||
| Active | 3.7% (2.2% to 5.1%) | 1.96 (1.16 to 3.31) | 2.13 (1.26 to 3.60) | |||
| Missing | 0% | n/a | n/a | |||
| Anterior chamber cells b , d | <.01 | .02 | ||||
| Quiet | 2.8% (1.8% to 3.8%) | Reference | Reference | |||
| 0.5+ | 1.6% (0.3% to 2.8%) | 0.55 (0.24 to 1.25) | 0.57 (0.25 to 1.33) | |||
| 1+ | 0.8% (0.0% to 2.0%) | 0.30 (0.07 to 1.22) | 0.30 (0.07 to 1.28) | |||
| 2+ or worse | 6.3% (2.3% to 10.2%) | 2.29 (1.16 to 4.55) | 2.13 (1.26 to 3.60) | |||
| Vitreous cells b , d | .79 | .89 | ||||
| Quiet | 3.0% (1.9% to 4.0%) | Reference | Reference | |||
| 0.5+ | 2.7% (1.2% to 4.1%) | 0.90 (0.49 to 1.64) | 0.96 (0.52 to 1.76) | |||
| 1+ | 2.7% (0.9% to 4.5%) | 0.92 (0.47 to 1.77) | 0.97 (0.48 to 1.93) | |||
| 2+ or worse | 1.9% (0.4% to 3.5%) | 0.65 (0.28 to 1.52) | 0.71 (0.31 to 1.64) | |||
| Missing | 0% | n/a | n/a | |||
| Vitreous haze b , d | .77 | .93 | ||||
| Quiet | 2.9% (2.0% to 3.8%) | Reference | Reference | |||
| 1+ | 2.2% (0.5% to 3.9%) | 0.76 (0.34 to 1.68) | 0.83 (0.37 to 1.86) | |||
| 2+ or worse | 1.6% (0.0% to 4.0%) | 0.55 (0.13 to 2.42) | 0.69 (0.15 to 3.11) | |||
| Missing | 2.2% (0.0% to 4.4%) | 0.75 (0.26 to 2.16) | 0.84 (0.29 to 2.48) | |||
| Use of any immunomodulatory treatment d , e | .89 | .72 | ||||
| No | 2.7% (1.6% to 3.7%) | Reference | Reference | |||
| Yes | 2.7% (1.7% to 3.8%) | 1.04 (0.64 to 1.67) | 1.09 (0.68 to 1.75) | |||
| Bilateral uveitis | .12 | .04 | ||||
| No | 204 | 4.4% (1.4% to 7.3%) | Reference | Reference | ||
| Yes | 2160 | 2.6% (1.7% to 3.4%) | 0.57 (0.28 to 1.16) | 0.40 (0.18 to 0.88) | ||
| Prior contralateral CNV d | <.01 | <.01 | ||||
| No | 2.4% (1.7% to 3.2%) | Reference | Reference | |||
| Yes | 17.2% (6.6% to 26.5%) | 7.66 (4.06 to 14.46) | 5.79 (2.77 to 12.09) |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


