Purpose
To identify risk factors for local recurrence and metastasis of sebaceous gland carcinoma (SGC) after wide excision with paraffin section control.
Design
Retrospective, observational case-control study.
Methods
Setting : Single institution. Patient Population : Thirty-four patients with SGC who had undergone excision with 5-mm surgical margins and paraffin section pathologic analysis. Observational Procedures : The following were considered potential risk factors for local recurrence/metastasis of SGC: patient’s sex, patient’s age, initial diagnosis at other clinics, topical treatments at other clinics, interval between appearance of symptoms and referral to our institution, tumor location, tumor origin, tumor presentation pattern, T category, tumor size, presence/or absence of pagetoid spread, tumor differentiation, mitosis grade, growth pattern. Logistic regression analysis was performed to identify the actual risk factors. Main Outcome Measures : Risk factors for local recurrence or metastasis of SGC after wide excision with paraffin section control.
Results
Involvement of both upper and lower eyelids, topical treatments at other clinics, multicentric origin, diffuse pattern, stage T3a, large tumor size, and a nonlobular pattern significantly influenced local recurrence/metastasis ( P < .050). Pagetoid spread tended to affect local recurrence/metastasis ( P = .052). The other items did not significantly influence local recurrence/metastasis ( P > .050).
Conclusions
This study identified risk factors for local recurrence or metastasis of SGC after wide excision with paraffin section pathologic analysis. The results of this study will be helpful to surgeons when planning additional management, such as map biopsy or adjuvant treatment.
Sebaceous gland carcinoma (SGC) is a malignancy of the eyelid that exhibits aggressive local behavior and metastasizes to regional lymph nodes and/or distant organs. These features result in considerable tumor-related mortality, accounting for 3%–41% of all patients with SGC.
Proper management is essential to reduce the risk of local recurrence/metastasis of SGC. Mohs micrographic surgery and wide excision with frozen-section control have been reported as reliable SGC management. An advantage of these surgeries is the ability to reconstruct an eyelid defect at 1 operative session. A specialist Mohs surgeon, however, is not always available. In addition, frozen-section control occasionally results in misinterpreting a specimen’s margin and overlooking pagetoid spread. Another useful management protocol for SGC is a procedure that combines excision with 3- to 5-mm surgical margins, paraffin section control, and delayed reconstruction. The accuracy of this method is similar to that of Mohs micrographic surgery using eyelid margin control.
Understanding the prognostic risk factors associated with SGC enables surgeons to plan additional management, such as map biopsy and adjuvant treatment. Previously reported prognostic risk factors include misdiagnosing SGC as another, benign lesion ; a prolonged interval from symptom appearance to the correct diagnosis ; tumor location ; tumor origin ; the T category, as defined by the American Joint Committee on Cancer (AJCC) ; tumor size ; pagetoid spread ; tumor differentiation ; and the tumor’s growth pattern. These previous studies, however, included patients who had had some adjuvant chemotherapy or radiotherapy, patients with unknown management, and/or patients with metastasis prior to excision. None of the previous studies had directly investigated risk factors for local recurrence/metastasis of SGC solely after excision with pathologic management.
In this study, we examined the risk factors for local recurrence and metastasis of SGC after wide excision with paraffin section control.
Methods
Study Design, Setting, and Ethics Approval
This study was a retrospective chart review of all Japanese patients with SGC who underwent wide excision with paraffin section control between April 3, 2006 and September 1, 2015 at Aichi Medical University Hospital. This study was approved by the Institutional Review Board (IRB) of Aichi Medical University Hospital (No. 2016-016) and followed the tenets of the Declaration of Helsinki. The IRB granted a waiver of informed consent for this study on the basis of the ethical guidelines for medical and health research involving human subjects established by the Japanese Ministry of Education, Culture, Sports, Science, and Technology and the Ministry of Health, Labour, and Welfare. The waiver was granted because the study was a retrospective chart review, not an interventional study, and because it was difficult to obtain consent from patients who had been treated several years prior to this study. Nevertheless, at the request of the IRB, we published an outline of the study, available for public viewing on the Aichi Medical University Hospital website. This public posting also gave patients the opportunity to decline participation, although none of the patients did so. Personal identifiers were removed from the records prior to data analysis.
Patients with metastatic lesions at the first examination or a follow-up time <6 months were excluded from the study. None of the patients had a history of prior irradiation, retinoblastoma, Muir-Torre syndrome, diuretic use, immunosuppressive treatment, or human immunodeficiency virus infection.
Data Collection
The following patient data were collected: patient’s sex, patient’s age, initial diagnosis at other clinics, topical treatment at other clinics, and interval between appearance of symptoms and referral to our institution. Topical treatments included eye drops, ointment, curettage, and cryosurgery for blepharitis, chalazion, and other benign tumors.
The following clinicopathologic data were collected: tumor location, size, origin, and presentation pattern; T category; presence/absence of pagetoid spread; tumor differentiation; mitosis grade; and growth pattern. SGC originates from the meibomian glands, Zeis glands, lacrimal caruncle, pilosebaceous glands in the eyelid, conjunctiva, and/or multicentric regions. The tumor presents in nodular, diffuse, and pedunculated patterns. The T category was defined using the TNM (tumor–node–metastasis) criteria as outlined by the AJCC 7th edition guidelines. SGC was classified into 3 groups according to the degree of differentiation. Well-differentiated tumors had a nodular pattern with cells at the center of the lobules exhibiting sebaceous differentiation. Moderately differentiated tumors were predominantly composed of anaplastic cells, with only a few areas of highly differentiated sebaceous cells. Poorly differentiated tumors had cells with primarily pleomorphic nuclei, prominent nucleoli, and amphophilic-positive cytoplasm. Mitosis was classified into 3 groups: grade 1, 0–1/high-power field (HPF), magnification ×400; grade 2, 2–5/HPF; grade 3, >5/HPF. The tumor growth patterns included lobular, comedocarcinoma, papillary, and mixed.
Management
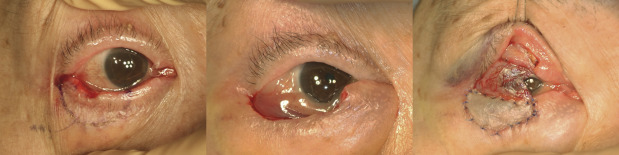
Two oculoplastic surgeons (Y.T., H.K.) performed the surgical procedures. If a pathologic diagnosis had not been obtained prior to referral to our institution, an incisional biopsy was performed at the first examination. Immediately after the pathologic diagnosis was obtained, the tumor was excised with 5-mm surgical margins ( Figure 1 , Left and Center). All surgical margins were pathologically confirmed with permanent paraffin section analysis using hematoxylin-eosin stain 1 week after the excision. In patients with pathologic findings in a gray zone, the specimens were stained using epithelial membrane antigen (EMA) (3 patients) and/or adipophilin (5 patients). When a residual tumor was found on the paraffin sections, an additional 5-mm-wide excision of the involved lesion was performed. This procedure was repeated until the margin sections were free of tumor. When a negative result was obtained in the margin sections, eyelid reconstruction was performed using a local flap, skin graft, and/or free tarsal graft ( Figure 1 , Right). None of the patients had undergone map biopsy or adjuvant cryotherapy, chemotherapy, or radiotherapy before the development of a local recurrence/metastasis.
All patients underwent a systemic computed tomographic evaluation at the first examination and at every 6-month follow-up visit for 3 years to check for metastatic lesions.
Review of the Margin Sections With Adipophilin
Adipophilin has recently become well recognized in the ophthalmic field as a useful immunohistochemical stain for SGC. For this study, all surgical margins were reviewed immunohistopathologically using adipophilin in patients with local recurrence/metastasis. The paraffin-embedded margin tissues were sliced and stained with primary antibodies against adipophilin (clone: AP125; Acris Antibodies, Inc, Rockville, Maryland, USA) in accordance with the manufacturer’s guidelines. Adipophilin immunostains were examined by light microscopy.
Statistical Analysis
The patient’s age, interval between the appearance of symptoms and referral to our institution, and tumor size were expressed as means ± standard deviations (SD) and were compared between patients with and without local recurrence/metastasis using the Mann-Whitney U test. Comparisons of the other parameters between patients with and without local recurrence/metastasis were carried out using the Pearson χ 2 test or Fisher exact probability test. For 2 × 2 tables, when the number of patients was <5, we used Fisher exact probability test. Logistic regression analysis was carried out to determine risk factors for local recurrence/metastasis of SGC. For the logistic regression analysis, all categorized factors were expressed using a binary system (a dummy variable, 0 and 1). The percentage of patients with local recurrence/metastasis was compared between the surgeons using Fisher exact probability test. All statistical analyses were performed using SPSS version 22 software (IBM Japan, Tokyo, Japan). P < .05 was considered to indicate statistical significance.
Results
The patients’ data, clinicopathologic findings, and statistical comparisons between patients with and without local recurrence/metastasis are shown in Tables 1 and 2 . Although 36 patients with SGC were referred to our institution, 2 patients were excluded from this study because they had metastasis to the parotid gland at the first examination. None of the patients had less than 6 months follow-up in this study. Altogether, 34 patients (17 men, 17 women; mean age 72.2 ± 12.3 years, range 34–96 years; 12 with right eyelid affected, 22 with left eyelid affected) were included in this study. The mean follow-up period was 43.7 ± 24.9 months (range 6–120 months).
| Parameter | Total | Local Recurrence/Metastasis | P | |
|---|---|---|---|---|
| + | − | |||
| Number of patients (male/female) | 34 (17/17) | 4 (2/2) | 30 (15/15) | 1.000 |
| Age, y (range) | 72.2 ± 12.3 (34–96) | 74.3 ± 7.8 (64–82) | 71.9 ± 12.8 (34–96) | .777 |
| Follow-up periods, mo (range) | 43.7 ± 24.9 (6–120) | 45.5 ± 25.0 (21–69) | 43.3 ± 25.3 (6–120) | .738 |
| Initial diagnosis at other clinics, n (%) | ||||
| Malignant tumor | 19 (55.9) | 1 (25.0) | 18 (60.0) | .010 |
| Benign lesion | 15 (44.1) | 3 (75.0) | 12 (40.0) | |
| Blepharitis | 5 (14.7) | 2 (50.0) | 3 (10.0) | |
| Chalazion | 7 (20.6) | 0 | 7 (23.3) | |
| Papilloma | 2 (5.9) | 0 | 2 (6.7) | |
| Blepharitis and seborrheic keratosis | 1 (2.9) | 1 (25.0) | 0 | |
| Patients who underwent topical treatments at other clinics, n (%) | 11 (32.4) | 3 (75.0) | 8 (26.7) | .089 |
| Duration from appearance of symptoms to referral to our institution, mo (range) | 12.8 ± 21.8 (1–120) | 11.0 ± 9.8 (1–24) | 13.0 ± 23.0 (1–120) | .699 |
| Findings | Total (n = 34) | Local Recurrence/Metastasis | P | |
|---|---|---|---|---|
| + (n = 4) | − (n = 30) | |||
| Location, n (%) | ||||
| Right | 12 (35.3) | 1 (25.0) | 11 (36.7) | 1.000 |
| Left | 22 (64.7) | 3 (75.0) | 19 (63.3) | |
| Upper eyelid | 22 (64.7) | 1 (25.0) | 21 (70.0) | .007 |
| Lower eyelid | 9 (26.5) | 1 (25.0) | 8 (26.7) | |
| Both upper and lower eyelids | 3 (8.8) | 2 (50.0) | 1 (3.3) | |
| Tumor origin, n (%) | ||||
| Meibomian gland | 25 (73.5) | 1 (25.0) | 24 (80.0) | .041 |
| Zeis gland | 1 (2.9) | 0 | 1 (3.3) | |
| Pilosebaceous gland | 1 (2.9) | 0 | 1 (3.3) | |
| Multicentric | 7 (20.6) | 3 (75.0) | 4 (13.3) | |
| Tumor presentation pattern, n (%) | ||||
| Nodule | 29 (85.3) | 1 (25.0) | 28 (93.3) | .006 |
| Diffuse | 5 (14.7) | 3 (75.0) | 2 (6.7) | |
| T category, a n (%) | ||||
| T2a | 24 (70.6) | 1 (25.0) | 23 (76.7) | .001 |
| T2b | 5 (14.7) | 0 | 5 (16.7) | |
| T3a | 5 (14.7) | 3 (75.0) | 2 (6.7) | |
| Tumor size, mm (range) | 9.7 ± 7.5 (3–30) | 23.8 ± 9.5 (10–30) | 7.9 ± 4.9 (3–20) | .002 |
| Pagetoid spread, n (%) | 11 (32.4) | 3 (75.0) | 8 (26.7) | .089 |
| Differentiation, n (%) | ||||
| Good | 13 (38.2) | 1 (25.0) | 12 (40.0) | .237 |
| Moderate | 8 (23.5) | 0 | 8 (26.7) | |
| Poor | 13 (38.2) | 3 (75.0) | 10 (33.3) | |
| Mitosis, n (%) | ||||
| 0–1/HPF | 19 (55.9) | 3 (75.0) | 16 (53.3) | .636 |
| 2–5/HPF | 4 (11.8) | 0 | 4 (13.3) | |
| >5/HPF | 11 (32.4) | 1 (25.0) | 10 (33.3) | |
| Growth pattern, n (%) | ||||
| Lobular | 24 (70.6) | 1 (25.0) | 23 (76.7) | .112 |
| Nonlobular | 10 (29.4) | 3 (75.0) | 7 (23.3) | |
| Comedocarcinoma | 4 (11.8) | 1 (25.0) | 3 (10.0) | |
| Lobular/comedocarcinoma | 5 (14.7) | 2 (50.0) | 3 (10.0) | |
| Lobular/papillary | 1 (2.9) | 0 | 1 (3.3) | |
Local recurrence/metastasis occurred in 4 patients ( Figure 2 ) during the postexcision period. There was no difference in the percentage of patients with local recurrence/metastasis between the surgeons ( P = 1.000). Patients with local recurrence/metastasis were more frequently misdiagnosed as having a benign lesion than those without local recurrence/metastasis ( P = .010). In addition, patients with local recurrence/metastasis exhibited different tumor locations ( P = .007), tumor origins ( P = .041), tumor presentation patterns ( P = .006), T categories ( P = .001), and tumor sizes ( P = .002) from patients without local recurrence/metastasis. Three of the 4 patients with local recurrence/metastasis had a tumor >20 mm in maximum diameter. All patients without local recurrence/metastasis had a tumor of ≤20 mm. This boundary corresponds to that of the basis of size to differentiate between stages T2b and T3a. We therefore defined a “large” tumor as one that is >20 mm in maximum diameter.
The detailed clinicopathologic data of the 4 patients with local recurrence/metastasis are shown in Table 3 . The interval between excision and recurrence/metastasis ranged from 5 to 27 months. Three of the 4 patients (Patients 1, 3, and 4) showed similar characteristics, such as misdiagnosis and topical treatment at other clinics, multicentric origin, diffuse and nonlobular patterns, tumors >20 mm in maximum diameter at stage T3a, pagetoid spread, and poor differentiation. These 3 patients had undergone additional treatment and were free from SGC at the last follow-up. The other patient (Patient 2) was hospitalized for malignant lymphoma treatment at another clinic immediately after metastasis to the parotid gland was diagnosed. The metastasis in this patient was managed at this clinic.
| Parameter | Patient 1 | Patient 2 | Patient 3 | Patient 4 |
|---|---|---|---|---|
| Sex | M | F | M | F |
| Age, y | 73 | 82 | 64 | 78 |
| Initial diagnosis at other clinics | Blepharitis/seborrheic keratosis | Malignant tumor | Blepharitis | Blepharitis |
| Topical treatment at other clinics | Ointment/cryosurgery | – | Ointment | Ointment |
| Duration from appearance of symptoms to referral to our clinic, mo | 12 | 1 | 7 | 24 |
| Location | ||||
| Right/left | L | R | L | L |
| Upper/lower | U/Lo | U | Lo | U/Lo |
| Tumor origin | Multicentric | Meibomian glands | Multicentric | Multicentric |
| Tumor presentation pattern | Diffuse | Nodule | Diffuse | Diffuse |
| T category a | T3a | T2a | T3a | T3a |
| Tumor size, mm | 30 | 10 | 25 | 30 |
| Pagetoid spread | + | − | + | + |
| Differentiation | Poor | Good | Poor | Poor |
| Mitosis | 0–1/HPF | 0–1/HPF | > 5/HPF | 0–1/HPF |
| Growth pattern | Lobular/comedoCa | Lobular | ComedoCa | Lobular/comedoCa |
| Local recurrence/metastasis | Metastasis to regional lymph node | Metastasis to parotid gland | Local recurrence in the medial lower eyelid margin | Local recurrence in the lateral lower eyelid margin |
| Duration from wide excision to local recurrence/metastasis, mo | 5 | 27 | 14 | 13 |
| Second management | Lymph node dissection | Management at another hospital | Wide excision | Wide excision plus topical mitomycin C + oral TS-1 b |
| Clinical course after second management | Local recurrence in the lateral upper eyelid margin and lacrimal gland invasion 10 months after 2nd surgery
| Unknown | Metastasis to parotid gland 12 months after 2nd surgery
| Free from SGC for 5 months |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


