Purpose
To compare the diagnostic abilities of the vessel densities in optic nerve head (ONH), peripapillary, and macular regions measured using optical coherence tomography angiography (OCTA) in eyes with primary open-angle glaucoma (POAG), and to evaluate the effect of glaucoma severity (based on the mean deviation, MD), optic disc size, and pretreatment intraocular pressure (IOP).
Design
Cross-sectional study.
Methods
Seventy-eight eyes of 53 control subjects and 64 eyes of 39 POAG patients underwent OCTA imaging. Area under receiver operating characteristic (ROC) curves (AUC) and sensitivities at fixed specificities of vessel densities in ONH, peripapillary, and macular regions were analyzed. ROC regression was used to evaluate the effect of covariates on the diagnostic abilities.
Results
The AUCs of ONH vessel densities ranged between 0.59 (superonasal sector) and 0.73 (average inside disc), peripapillary between 0.70 (nasal, superonasal and temporal) and 0.89 (inferotemporal), and macular between 0.56 (nasal) and 0.64 (temporal). AUC of the average peripapillary vessel density was significantly better than the average inside disc ( P = .05) and macular ( P = .005) measurement. MD showed a negative association with the AUCs of the vessel densities of all regions. Pretreatment IOP (coefficient: 0.09) showed a significant ( P < .05) effect on the AUC of ONH vessel density.
Conclusions
Diagnostic ability of the vessel density parameters of OCTA was only moderate. Macular and inside disc densities had significantly lower diagnostic abilities in POAG than the peripapillary density. Diagnostic abilities of vessel densities increased with increasing severity of glaucoma and that of ONH vessel density with higher pretreatment IOPs.
Primary open angle glaucoma (POAG) is a chronic progressive optic neuropathy resulting from the apoptosis of the retinal ganglion cells (RGC). Although the pathogenic mechanisms leading to retinal ganglion cell death are not fully known, intraocular pressure (IOP)–induced mechanical injury is a major causal factor, as evidenced by the increase in the risk of incident glaucoma and its progression with higher IOP. It has also been proposed that reduced optic nerve head (ONH) perfusion also plays a role in the pathogenesis of glaucoma. Although some believe that the reduced blood flow seen in glaucoma is secondary to RGC death and thereby a reduced need for perfusion, others are of the opinion that the reduced blood flow is the primary event that subsequently leads to the characteristic structural and functional changes of glaucoma. Earlier studies have measured ONH blood flow using a variety of techniques and have shown reduction in ONH perfusion in patients with glaucoma. However, each of these techniques has limitations.
Optical coherence tomography (OCT) has been used to develop a new, 3-dimensional angiography algorithm called split-spectrum amplitude-decorrelation angiography (SSADA) for imaging the retinal and ONH microcirculation. Early studies have shown that the blood flow measurements provided by OCT angiography (OCTA) are repeatable and reproducible. Studies with OCTA have demonstrated reduced ONH and peripapillary perfusion in patients with glaucoma. OCTA also evaluates the vascular perfusion in the macular region. However, there have been no reports on the macular perfusion in patients with glaucoma. There have not been comparisons to date of the diagnostic abilities of vessel densities in the ONH, peripapillary, and macular regions in glaucoma. The purpose of this study was to compare the diagnostic abilities of the vessel density measurements of the ONH, peripapillary, and macular regions on OCTA in eyes with POAG. The secondary objective was to evaluate the effect of glaucoma severity, optic disc size, and the pretreatment IOP on the diagnostic abilities of vessel densities.
Methods
This was a cross-sectional study conducted at Narayana Nethralaya, a tertiary eye care center in Bengaluru, South India, between September 2015 and March 2016. The methodology adhered to the tenets of the Declaration of Helsinki for research involving human subjects. Written informed consent was obtained from all participants and the study was approved by the Institute’s Ethics Committee.
Participants of the study included control subjects and POAG patients. Control subjects were either hospital staff or subjects who consulted for a routine eye examination or a refractive error. Control subjects had no family history of glaucoma, IOP≤21 mm Hg, normal anterior and posterior segment on clinical examination by an ophthalmologist, and nonglaucomatous optic discs, as assessed by experts on masked examination of stereoscopic optic disc photographs. POAG patients had open angles on gonioscopy and glaucomatous changes on optic nerve head examination (neuroretinal rim narrowing, notching, and retinal nerve fiber layer defects), as documented by glaucoma experts on dilated examination and confirmed by experts on stereoscopic optic disc photographs. Inclusion criteria for all participants were age ≥18 years, corrected distance visual acuity of 20/40 or better, and refractive error within ±5 diopters (D) sphere and ±3 D cylinder. Exclusion criteria were presence of any media opacities that prevented good-quality OCT scans, or any retinal or neurological disease other than glaucoma, which could confound the evaluation. Eyes with a history of trauma or inflammation were also excluded. All participants underwent a comprehensive ocular examination, which included a detailed medical history, corrected distance visual acuity measurement, slit-lamp biomicroscopy, Goldmann applanation tonometry, gonioscopy, dilated fundus examination, visual field (VF) examination, and OCTA imaging with RTVue-XR spectral-domain (SD) OCT (Optovue Inc, Fremont, California, USA). Baseline (pretreatment) IOP, the IOP at which anti-glaucoma treatment was started, was documented for all POAG eyes.
Stereoscopic optic disc photographs were obtained by trained technicians using a digital fundus camera (Kowa nonmyd WX; Kowa Company Ltd., Tokyo, Japan). Each optic disc photograph was evaluated independently by 2 glaucoma experts (H.L.R. and N.K.P.) in a masked manner to determine the presence of glaucomatous changes (focal or diffuse neuroretinal rim thinning, localized notching, or retinal nerve fiber layer defects). The experts were masked to all the clinical data, visual field data, and the other-eye data. Discrepancy in the classification between the 2 experts was adjudicated by a third glaucoma expert (Z.S.P.).
VF examination was performed using a Humphrey Field Analyzer II, model 720i (Zeiss Humphrey Systems, Dublin, California, USA), with the Swedish interactive thresholding algorithm (SITA) standard 24-2 program. VFs were considered reliable if the fixation losses were less than 20% and the false-positive and false-negative response rates were less than 15%. VF result was not considered for the definition of glaucoma or the controls but was used for the grading of glaucoma severity.
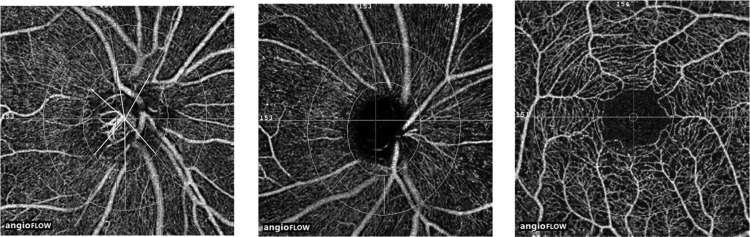
OCTA imaging of the optic disc, peripapillary region, and macula was performed using RTVue-XR SDOCT (AngioVue, v2015.100.0.33). RTVue-XR uses an 840 nm diode laser source, with an A-scan rate of 70 kHz per second. Imaging is performed using a set of 2 scans: 1 vertical-priority and 1 horizontal-priority raster volumetric scan. The optic disc scan covers an area of 4.5 × 4.5 mm and the macular scan was performed using volumetric scans covering 3 × 3 mm. An orthogonal registration algorithm is used to produce merged 3-dimensional OCT angiograms. The SSADA algorithm compares the consecutive B-scans at the same location to detect flow using motion contrast. Vessel densities are calculated over the entire scan area (ie, whole en face disc and whole en face macula). Vessel density is defined as the percentage area occupied by the large vessels and microvasculature in a particular region. In addition to the whole-scan analysis, the software calculates vessel densities in various layers of the retina and the ONH, and each scan region is further divided into sectors as described below. An en face angiogram of the ONH and peripapillary circulation is obtained by the maximum flow (decorrelation value) projection from the inner limiting membrane (ILM) to retinal pigment epithelium (RPE). The ONH vessel densities were calculated from the “nerve head” segment of the ONH angiogram ( Figure 1 , Left). This segment extends from 2000 μm above the ILM to 150 μm below the ILM. The software automatically fits an ellipse to the optic disc margin and calculates the average vessel density within the ONH (referred to as the inside disc vessel density). It also divides the ONH into 6 sectors based on the Garway-Heath map and calculates the vessel densities in each ONH sector (nasal, inferonasal, inferotemporal, superotemporal, superonasal, and temporal sectors), as represented in Figure 1 , Left. The peripapillary region is defined as a 0.75-mm-wide elliptical annulus extending from the optic disc boundary ( Figure 1 , Middle). The peripapillary vessels were analyzed in superficial retinal layers from the radial peripapillary capillary (RPC) segment. The RPC segment extends from the ILM to the nerve fiber layer. The peripapillary region was also divided into 6 sectors based on the Garway-Heath map ( Figure 1 , Middle) and vessel densities for the entire peripapillary area (average) and each sector were determined. Macular vessel densities analyzed in this study were of the superficial vascular plexus present in the inner layers of the retina (extending from the ILM to the inner plexiform layer). Macular vessel densities were analyzed over a 1.5-mm-wide parafoveal, circular annulus centered on the macula ( Figure 1 , Right). The parafoveal region was also divided into 4 sectors of 90 degrees each (nasal, inferior, superior, and temporal sectors). Image quality was assessed for all OCTA scans. Poor-quality images with a signal strength index (SSI) less than 35 or images with residual motion artifacts were excluded from the analysis.
All subjects also underwent optic disc area measurement on RTVue-XR SDOCT using the traditional ONH scan. This scan consists of 12 radial scans 3.4 mm in length and 6 concentric ring scans ranging from 2.5 to 4.0 mm in diameter, all centered on the optic disc. RPE tips are automatically detected by the software and the RPE tips are joined to delineate the optic disc margin and to calculate the disc area. All the examinations for a particular subject were performed on the same day.
Statistical Analysis
Descriptive statistics included mean and standard deviation for normally distributed variables and median and interquartile range (IQR) for non-normally distributed variables. Shapiro-Wilk test was used to test for the normality distribution of continuous variables. Receiver operating characteristic (ROC) curves were used to describe the ability of OCTA vessel densities to discriminate glaucomatous eyes from control eyes. Sensitivities at fixed specificities of 80% and 95% were determined for all the parameters. To obtain confidence intervals for area under the ROC curves (AUC) and sensitivities, a bootstrap resampling procedure was used (n = 1000 resamples). Because measurements from both eyes of the same subject are likely to be correlated, the standard statistical methods for parameter estimation lead to underestimation of standard errors and to confidence intervals that are too narrow. Therefore, the cluster of data for the study subject was considered as the units of resampling and bias-corrected standard errors were calculated during all estimations. This procedure has been used to adjust for the presence of multiple correlated measurements from the same unit. The ROC regression modeling technique was used to evaluate the effect of glaucoma severity, disc size, and the pretreatment IOP on the AUCs and sensitivities of OCTA parameters in diagnosing glaucoma.
Statistical analyses were performed using commercial software (Stata ver. 13.1; StataCorp, College Station, Texas, USA). A P value of ≤.05 was considered statistically significant.
Results
One hundred and seventy-one eyes of 102 subjects (86 eyes of 56 subjects diagnosed as normal and 85 eyes of 46 subjects diagnosed as POAG on clinical examination) underwent OCTA imaging with SDOCT. Among these, 19 eyes of 13 patients, in which the optic disc classification on stereophotographs was not glaucomatous optic neuropathy, were excluded. In addition, 20 poor quality disc scans and 25 poor quality macular scans (10 eyes had poor quality of both disc and macular scans) were also excluded. Final analysis included 132 optic disc scans and 127 macular scans obtained from 142 eyes of 92 subjects (78 eyes of 53 normal and 64 eyes of 39 POAG subjects). Of the 64 eyes with POAG, 12 eyes (11 patients) had a “within normal limit” or a “borderline” glaucoma hemifield test result or the probability value of pattern standard deviation >5% or both on VF (preperimetric glaucoma). Half the number of eyes included in the POAG group had a mean deviation of better than −5 dB on VF. Of the 64 eyes with POAG, 13 eyes were on topical beta blockers, 10 on alpha agonists, 13 on carbonic anhydrase inhibitors, and 41 on prostaglandin analogues (either as a monotherapy or as components of the combination therapy). Table 1 shows the clinical, VF, and vessel density measurements of all subjects. POAG patients were significantly older than control subjects. SSI of the optic disc scans was significantly greater in the control as compared with the POAG patients. AUCs and sensitivities at fixed specificities of optic disc and peripapillary vessel density parameters were therefore calculated after adjusting for the difference in age and signal strength between the control and POAG groups using covariate adjustment as proposed by Pepe. AUCs and sensitivities at fixed specificities of macular vessel density parameters were similarly calculated after adjusting for the difference in age. All the ONH, peripapillary, and macular vessel densities were significantly lesser in the glaucoma compared with the control group. The magnitude of difference in the median vessel densities between the glaucoma and the control groups was significantly smaller in the macular region compared with the ONH and peripapillary regions.
| Control Group (78 Eyes, 53 Subjects) | POAG Group (64 Eyes, 39 Patients) | P | |
|---|---|---|---|
| Age (y) | 58 (52, 65) | 66 (57, 72) | .01 |
| Sex (male:female) | 29:24 | 28:11 | .10 |
| Sphere (D) | 0.5 (0, 1) | 0 (−0.75, 0.5) | .02 |
| Cylinder (D) | −0.5 (−1, −0.5) | −0.75 (−1, −0.25) | .67 |
| Optic disc area (mm 2 ) | 2.30 (2.00, 2.58) | 2.33 (1.98, 2.59) | .93 |
| Pretreatment IOP (mm Hg) | 16 (14, 18) | 19 (16, 24) | <.001 |
| Hypertension (yes:no) | 16:37 | 16:23 | .28 |
| Diabetes mellitus (yes:no) | 15:38 | 9:30 | .57 |
| Mean deviation (dB) | −1.1 (−3.0, −0.2) | −5.3 (−9.6, −3.1) | <.001 |
| Pattern standard deviation (dB) | 1.7 (1.5, 2.5) | 4.7 (2.8, 9.2) | <.001 |
| Visual field index (%) | 99 (98, 99) | 90 (75, 95) | <.001 |
| SSI (optic disc scan) a | 54.2 ± 9.5 | 50.4 ± 8.2 | .02 |
| Whole en face vessel density (disc scan) | 54.4 (51.7, 56.9) | 48.0 (42.9, 53.4) | <.001 |
| Inside disc vessel density | 47.4 (43.0, 50.4) | 40.2 (34.8, 47.3) | <.001 |
| Nasal vessel density (%) | 48.8 (42.9, 52.5) | 41.6 (35.8, 47.6) | <.001 |
| Inferonasal vessel density (%) | 51.9 (44.8, 56.7) | 47.5 (39.9, 53.8) | .008 |
| Inferotemporal vessel density (%) | 46.2 (41.1, 52.3) | 39.7 (33.4, 47.5) | <.001 |
| Superotemporal vessel density (%) | 47.6 (41.9, 52.0) | 39.5 (28.3, 47.2) | <.001 |
| Superonasal vessel density (%) | 50.1 (42.9, 55.2) | 43.7 (37.2, 52.1) | .004 |
| Temporal vessel density (%) | 44.5 (39.1, 52.3) | 36.2 (28.7, 45.4) | <.001 |
| Average peripapillary vessel density (%) | 62.0 (60.0, 64.4) | 55.5 (50.8, 59.5) | <.001 |
| Nasal vessel density (%) | 59.7 (57.2, 62.1) | 56.0 (48.7, 59.6) | <.001 |
| Inferonasal vessel density (%) | 63.4 (60.7, 66.5) | 55.2 (46.2, 60.6) | <.001 |
| Inferotemporal vessel density (%) | 66.0 (63.5, 68.4) | 55.5 (44.5, 59.9) | <.001 |
| Superotemporal vessel density (%) | 66.6 (64.0, 68.8) | 59.4 (53.4, 65.4) | <.001 |
| Superonasal vessel density (%) | 62.9 (56.5, 66.1) | 55.3 (48.7, 61.2) | <.001 |
| Temporal vessel density (%) | 60.4 (57.9, 64.2) | 57.0 (50.6, 60.1) | <.001 |
| SSI (macula scan) a | 62.0 ± 6.9 | 60.6 ± 7.7 | .28 |
| Whole en face vessel density (macula scan) | 48.3 (45.9, 50.3) | 44.7 (41.8, 47.6) | <.001 |
| Foveal vessel density (%) | 25.5 (22.9, 27.7) | 24.9 (22.3, 27.8) | .58 |
| Parafoveal vessel density (%) | 49.8 (47.7, 52.7) | 47.5 (44.7, 50.2) | <.001 |
| Nasal vessel density (%) | 48.5 (46.7, 51.1) | 47.0 (44.1, 48.9) | .01 |
| Inferior vessel density (%) | 51.6 (48.1, 53.9) | 48.9 (44.8, 51.7) | .001 |
| Superior vessel density (%) | 50.8 (48.2, 53.3) | 47.6 (45.0, 52.0) | .002 |
| Temporal vessel density (%) | 49.8 (47.5, 52.5) | 47.3 (45.0, 50.1) | .001 |
The AUCs and sensitivities at fixed specificities of the vessel density measurements to differentiate POAG from control eyes are shown in Table 2 . The AUCs of ONH vessel densities ranged between 0.59 (superonasal sector) and 0.73 (average inside disc density). Sensitivities at 95% specificity ranged between 11% (superotemporal sector) and 25% (inside disc density). The AUCs of peripapillary vessel densities ranged between 0.70 (nasal, superonasal, and temporal sector) and 0.89 (inferotemporal sector), and macular vessel densities ranged between 0.56 (nasal sector) and 0.64 (temporal sector). The sensitivities at 95% specificity of peripapillary vessel densities ranged between 25% (superonasal sector) and 68% (inferotemporal sector), and macular vessel densities ranged between 3% (nasal sector) and 15% (superior sector). The parameters with the highest diagnostic abilities were the whole en face vessel density of the disc scan (AUC of 0.90) and the inferotemporal sector peripapillary vessel density (AUC of 0.89). Figure 2 shows the ROC curves of the vessel density measurements of the inside disc, average peripapillary, and parafoveal regions. AUC of average peripapillary vessel density was significantly better than that of the inside disc ( P = .05) and the parafoveal ( P = .005) measurements. AUC of the inside disc vessel density was comparable to that of the average parafoveal vessel density ( P = .31).
| Vessel Density | AUC | Sensitivity at 95% Specificity | Sensitivity at 80% Specificity |
|---|---|---|---|
| Whole (disc scan) | 0.90 (0.81–0.95) | 67% (39–84) | 82% (62–92) |
| Inside disc | 0.73 (0.61–0.84) | 25% (04–52) | 57% (39–75) |
| Nasal | 0.70 (0.57–0.80) | 22% (04–49) | 54% (27–68) |
| Inferonasal | 0.61 (0.49–0.72) | 13% (03–28) | 43% (24–66) |
| Inferotemporal | 0.64 (0.53–0.74) | 13% (03–26) | 40% (21–56) |
| Superotemporal | 0.71 (0.60–0.81) | 11% (02–21) | 48% (32–67) |
| Superonasal | 0.59 (0.47–0.70) | 16% (04–32) | 24% (08–42) |
| Temporal | 0.67 (0.53–0.78) | 13% (02–42) | 48% (16–67) |
| Average peripapillary | 0.83 (0.74–0.90) | 47% (29–60) | 72% (49–86) |
| Nasal | 0.70 (0.56–0.81) | 27% (13–40) | 52% (31–77) |
| Inferonasal | 0.81 (0.73–0.88) | 53% (37–73) | 67% (49–81) |
| Inferotemporal | 0.89 (0.81–0.94) | 68% (45–81) | 78% (62–90) |
| Superotemporal | 0.76 (0.66–0.84) | 33% (14–45) | 58% (41–75) |
| Superonasal | 0.70 (0.59–0.80) | 25% (12–41) | 50% (30–67) |
| Temporal | 0.70 (0.59–0.80) | 28% (05–48) | 50% (35–68) |
| Whole en face (macula scan) | 0.69 (0.56–0.79) | 20% (02–51) | 54% (38–73) |
| Parafoveal | 0.63 (0.48–0.75) | 09% (02–28) | 34% (12–52) |
| Nasal | 0.56 (0.42–0.69) | 03% (01–20) | 31% (09–52) |
| Inferior | 0.61 (0.48–0.73) | 10% (02–46) | 37% (11–52) |
| Superior | 0.63 (0.50–0.74) | 15% (05–43) | 39% (16–63) |
| Temporal | 0.64 (0.50–0.77) | 07% (02–26) | 39% (14–64) |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


