Purpose
To investigate genetic, environmental, and systemic risk factors in prospectively identified subjects with the age-related macular degeneration (AMD) phenotypes of (1) reticular pseudodrusen without large soft drusen and (2) large soft drusen without reticular pseudodrusen.
Design
Prospective case-case comparison.
Methods
In a clinical practice setting, patients with AMD were sequentially screened using clinical examination and scanning laser ophthalmoscopy imaging to prospectively identify subjects (n = 73) with the phenotypes of (1) reticular pseudodrusen without large soft drusen (n = 30) or (2) large soft drusen without reticular pseudodrusen (n = 43). Subjects were genotyped for 2 alleles associated with AMD, age-related maculopathy susceptibility 2 ( ARMS2 ) and complement factor H ( CFH ). A questionnaire was administered to collect history of smoking, hypertension, diabetes, and hyperlipidemia, as well as personal and family history of AMD.
Results
The reticular pseudodrusen group was older (median age 87 vs 81 years, P = .04) and had more female subjects (83.3% vs 48.8%, P = .003), later ages of AMD onset (83 vs 70 years, P = .0005), and a greater frequency of hypertension (76.7% vs 55.8%, P = .08). No significant differences were found in the distribution of the ARMS2 risk allele ( P = .4) between the reticular pseudodrusen (homozygous = 20.0%; heterozygous = 56.7%) and large soft drusen (homozygous = 19.0%; heterozygous = 42.9%) phenotypes, or in the distribution of the CHF risk allele ( P = .7) between the reticular pseudodrusen (homozygous = 26.7%; heterozygous = 56.7%) and large soft drusen (homozygous = 21.4%; heterozygous = 66.7%) phenotypes.
Conclusions
The reticular pseudodrusen phenotype was associated with increased age, later age of AMD onset, and female sex.
Age-related macular degeneration (AMD) is the leading cause of adult blindness in industrialized countries, with a reported 1.47% prevalence and 1.75 million people affected in the United States alone. Both “wet” AMD, otherwise known as choroidal neovascularization (CNV), and geographic atrophy (GA), the advanced “dry” form of AMD, are considered advanced AMD. Although anti–vascular endothelial growth factor therapy is currently available to treat CNV, there are no proven forms of therapy for GA. Initially, antioxidants and vitamins were suggested as a preventative therapy for those with signs of “dry” AMD; however, later analysis by the Age-Related Eye Disease Study Research Group demonstrated that this therapy has no real effect on GA progression. Therefore, it is important to characterize “dry” AMD to elucidate its natural history and facilitate advancements in treatment and outcomes.
Drusen, concentrated deposits of extracellular material found around the macula, are an established marker for AMD. A different lesion type has been characterized and associated with AMD. Mimoun and associates first described “les pseudodrusen bleus” in 1990, referring to indistinct, interlacing yellowish lesions in the outer macula that are enhanced by blue light. These were considered a type of drusen and were included in the Wisconsin Age-Related Maculopathy Grading System as a separate entity called “reticular drusen,” based on their characteristic appearance. However, initial histopathologic analysis suggested that these lesions are associated with a loss of choroidal layers of small vessels and increased spacing between large choroidal veins not typical of AMD-associated drusen.
Reticular drusen, otherwise referred to as “reticular pseudodrusen,” are difficult to visualize using color fundus photography; therefore, since the development of scanning laser ophthalmoscope (SLO) imaging, including autofluorescence (AF) scans, near-infrared reflectance (NIR) scans, and indocyanine green angiography, these lesions have been more clearly characterized. Notable spatial correspondence of individual lesions using different imaging modalities was observed; from this observation, it was concluded that perhaps a single disease entity is responsible. The term “reticular macular disease” was defined as reticular pseudodrusen in color or red-free photography and/or a reticular pattern on SLO imaging. Spectral-domain optical coherence tomography (SD OCT) scans further extended the phenotypic characterization and, with histology, suggested anatomic correlation with lesions in the subretinal space, known as “subretinal drusenoid deposits.” The etiology of these lesions and the etiology of reticular pseudodrusen remain unclear. Other histopathologic and blood flow studies of AMD describe degenerative changes in the choriocapillaris and choroidal circulation insufficiency, and multimodal imaging of patients with reticular lesions has suggested an alteration in choriocapillaris blood flow.
There may be genetic risk factors for the reticular pseudodrusen subtype of AMD. Two major AMD risk alleles have been identified through genome-wide scanning and the candidate gene approach. In a retrospective study, 1 of the 2 major AMD risk alleles, complement factor H ( CFH , rs1061170) 402H, was less associated with reticular pseudodrusen than with the absence of reticular pseudodrusen (39.6% frequency in AMD with reticular pseudodrusen vs 58.6% in AMD without reticular pseudodrusen, P = .003). The other major risk allele, age-related maculopathy susceptibility 2 ( ARMS2 , rs10490924) 69S, was associated with an enhanced risk of reticular pseudodrusen (44.0% frequency in AMD with reticular pseudodrusen vs 31.3% in AMD without reticular pseudodrusen, P = .045). In a larger study, no significant difference was found in the frequency of either risk allele between eyes with AMD and reticular pseudodrusen and eyes with AMD and no reticular pseudodrusen.
While patients with reticular pseudodrusen make up only about 7%–8% of patients with AMD, as many as 32% of patients with CNV and 21% of patients with GA were found to have reticular pseudodrusen on color fundus photography. In another study, reticular pseudodrusen were found in more than 60% of patients with AMD on AF imaging, implying that the prevalence of reticular pseudodrusen may be higher than previously recognized ; and more recently, reticular pseudodrusen were found in over 90% of patients with GA. Interestingly, reticular pseudodrusen have been associated not only with both forms of late AMD, particularly with conversion to CNV, but also with female sex, systemic disease, and increased mortality.
The etiology of reticular pseudodrusen is unclear. Recent discoveries suggest that this AMD phenotype is complex and multifactorial, with possible genetic, environmental, and systemic factors. We hypothesize that this is indeed the case, as previous epidemiologic studies have suggested that reticular pseudodrusen are associated with cardiovascular risk factors and the ARMS2 risk allele. This study aimed to investigate genetic, environmental, and systemic risk factors in prospectively identified subjects with AMD and the phenotypes of (1) reticular pseudodrusen without large soft drusen and (2) large soft drusen without reticular pseudodrusen.
Methods
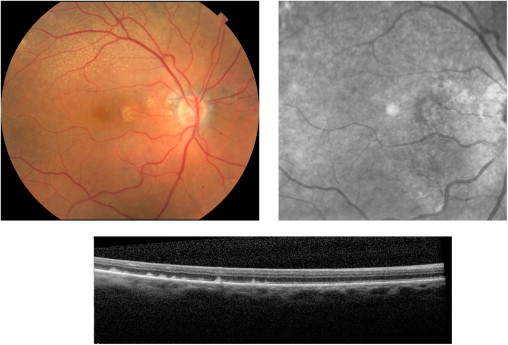
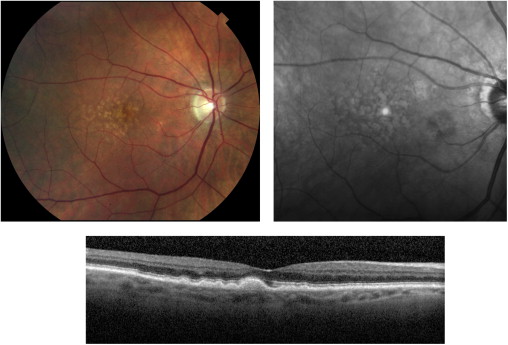
This prospective cross-sectional study was carried out with approval from the Institutional Review Board of New York University School of Medicine and in accordance with the Health Insurance Portability and Accountability Act of 1996. Informed consent, obtained from all study participants, included consent for participation in the study and permission to review relevant medical records. Between July 2012 and February 2013, study participants were recruited from 2 clinicians’ practices (K.B.F. and R.T.S.) and identified using clinical examination, SD OCT imaging, and SLO imaging with characteristics and methods as described previously. Briefly, NIR images were obtained using a confocal SLO (Spectralis; Heidelberg Engineering, Inc, Vista, California, USA). Two independent graders (S.B. and M.M.) detected reticular pseudodrusen on IR imaging as groups of hyporeflectant lesions against a mildly hyper-reflectant background, in well-defined and regular patterns, and confirmed reticular pseudodrusen by the presence of subretinal drusenoid deposits on SD OCT imaging obtained with the same instrument ( Figure 1 ). Large (≥125 μm) soft drusen were identified on color photographs by their characteristic yellow, indistinct appearance and confirmed by the presence of mounds of deposits under the retinal pigment epithelium on SD OCT imaging ( Figure 2 ). Any discrepancies were resolved by a senior grader (K.B.F. or R.T.S.). Based on these findings, patients were classified into 2 study groups: (1) subjects with an AMD phenotype of reticular pseudodrusen without large soft drusen and (2) subjects with an AMD phenotype of large soft drusen without reticular pseudodrusen.
Accordingly, inclusion criteria were AMD and a phenotype of reticular pseudodrusen without large soft drusen or AMD and a phenotype of large soft drusen without reticular pseudodrusen. Exclusion criteria were media opacity that resulted in poor image quality, photographic artifacts, or history of retinal vascular occlusion, retinal detachment, vitreoretinal or glaucoma surgery, retinal pigment epithelium tear, macular hole, central serous chorioretinopathy, or high myopia (spherical equivalent greater than −6 diopters).
All patients completed an extensive questionnaire that collected demographic information (age, race, and sex), personal and family history of AMD, smoking history, and history of cardiovascular risk factors, including hypertension, diabetes, and hyperlipidemia, as well as the use of medications being used to control these conditions. Elicited personal history of AMD included the age at diagnosis. A patient was defined as having a family history of AMD if he or she had any genetically related family member with AMD. Smoking history included ascertaining if the patient had ever smoked cigarettes for a total duration of 6 months or more. Hypertension was defined as having been previously diagnosed with elevated arterial blood pressure, which is being controlled by at least 1 hypertensive medication. Hyperlipidemia was defined as having been previously diagnosed with elevated blood lipid levels, which are being controlled by medication. Diabetes mellitus was defined as having been previously diagnosed with elevated blood glucose, which is being controlled by diet or medication.
Definitive CFH and ARMS2 genotyping was performed on all patients as follows: DNA was screened for haplotype-tagging single nucleotide polymorphisms in CFH (Y402H, rs1061170) and ARMS2 (A69S, rs10490924). Genotyping was performed using polymerase chain reaction–restriction fragment length polymorphism analysis using a master mix (Applied Biosystems; Life Technologies, Norwalk, Connecticut, USA). The thermal cycling conditions consisted of an initial hold at 95 C for 10 minutes, followed by 40 cycles of a 15-second 92 C denaturation step and a 1-minute 60 C annealing and extension step. Results were acquired using Applied Biosystems ViiA 7 RUO Software (Life Technologies).
Allele frequencies were compared between the 2 study groups. We used the nonparametric Kruskal-Wallis test to evaluate differences of quantitative variables between the 2 groups. For categorical variables, we report odds ratios (ORs) and 95% confidence intervals (CIs), with P values calculated from the χ 2 test or Fisher exact test. Age and age at AMD onset were analyzed both as continuous variables and as categorical variables, derived by dividing the overall distribution into tertiles. For ordinal variables, we used the Mantel test for trend to statistically test for evidence of increasing risk with increasing values. We performed multivariable analysis using exact logistic regression as implemented in PROC LOGISTIC (SAS 9.3, 2002–2010; SAS Institute, Inc, Cary, North Carolina, USA).
Results
Thirty patients with a phenotype of reticular pseudodrusen and no evidence of large soft drusen and 43 patients with a phenotype of large soft drusen and no evidence of reticular pseudodrusen were classified, with an inter-observer grading concordance of 90%, and enrolled in the study. The median age of patients included in the analysis was 87 years in the reticular pseudodrusen group and 81 years in the soft drusen group ( P = .04). Patients with reticular pseudodrusen also had a significantly later age of AMD onset than patients with soft drusen (83 years vs 70 years, respectively, P = .0005). The final analysis set comprised 46 women (46/73, 60.9%), with a significantly larger proportion of female subjects in the reticular pseudodrusen group than in the soft drusen group (25/30 [83.3%] vs 21/43 [48.8%], respectively, P = .003). All patients with soft drusen (43/43, 100%) and most patients with reticular pseudodrusen (29/30, 96.7%) were of European ancestry; 10 of 30 patients (33.3%) in the reticular pseudodrusen group and 9 of 43 patients (20.9%) in the soft drusen group reported an immediate family member with AMD ( P = .3). The distribution of the ARMS2 risk allele did not significantly differ ( P = .4) between the reticular pseudodrusen (homozygous = 20.0%; heterozygous = 56.7%) and the large soft drusen (homozygous = 19.0%; heterozygous = 42.9%) phenotypes. Similarly, the distribution of the CHF risk allele did not significantly differ ( P = .7) between the reticular pseudodrusen (homozygous = 26.7%; heterozygous = 56.7%) and the large soft drusen (homozygous = 21.4%; heterozygous = 66.7%) phenotypes ( Table 1 ).
| AMD With RPD and Without Large Soft Drusen, n (%) | AMD With Large Soft Drusen and Without RPD, n (%) | P Value | |
|---|---|---|---|
| Sex | .003 a | ||
| Male | 5 (16.7) | 22 (51.2) | |
| Female | 25 (83.3) | 21 (48.8) | |
| Race | .4 a | ||
| Non-Hispanic white | 29 (96.7) | 43 (100.0) | |
| Hispanic | 1 (3.4) | 0 (0.0) | |
| Age (y), median (q1–q3) | 87 (81–89) | 81 (74–88) | .04 b |
| Categorical age (y) | .02 c | ||
| ≤80 | 6 (20.0) | 19 (44.2) | |
| 81–86 | 7 (23.3) | 13 (30.2) | |
| ≥87 | 17 (56.7) | 11 (25.6) | |
| Age at AMD onset (years), median (q1–q3) | 83 (77–86) | 70 (66–78) | .0005 b |
| Categorical age at AMD onset (y) | .0006 c | ||
| ≤70 | 3 (10.0) | 22 (51.2) | |
| 71–82 | 12 (40.0) | 12 (27.9) | |
| ≥83 | 15 (50.0) | 9 (20.9) | |
| Years since AMD diagnosis, median (q1–q3) | 3 (2–6) | 7 (4–11) | .002 b |
| Family member with AMD | 10 (33.3) | 9 (20.9) | .3 a |
| Hypertension | .08 a | ||
| No | 7 (23.3) | 19 (44.2) | |
| Yes | 23 (76.7) | 24 (55.8) | |
| ARMS2 d risk allele (rs10490924) | .4 a | ||
| −/− | 7 (23.3) | 16 (38.1) | |
| +/− | 17 (56.7) | 18 (42.9) | |
| +/+ | 6 (20.0) | 8 (19.0) | |
| CFH e risk allele (rs1061170) | .7 a | ||
| −/− | 5 (16.7) | 5 (11.9) | |
| +/− | 17 (56.7) | 28 (66.7) | |
| +/+ | 8 (26.7) | 9 (21.4) |
a P value from Fisher exact test.
c P value from the Mantel test for trend.
d ARMS2 (age-related maculopathy susceptibility 2 gene) genotyping for 1 individual with large soft drusen was indeterminate and is not shown in these data.
e CFH (complement factor H gene) genotyping for 1 individual with large soft drusen was indeterminate and is not shown in these data.
In Table 2 , we show univariable analyses of risk factors for reticular pseudodrusen, presenting the total sample of patients with AMD as having different values for (or presence/absence of) each factor. For each risk factor, we show the frequency and percentage of patients with reticular pseudodrusen, as well as ORs and 95% CIs for reticular pseudodrusen among those with a particular value of the risk factor compared to the reference group of those without the risk factor. ORs for reticular pseudodrusen associated with the ARMS2 and CFH risk alleles were not significantly different from the null value of 1.0. ORs for reticular pseudodrusen were significantly increased among older patients and patients with later ages of AMD onset; the test for trend was significant in both cases.
| Risk Factor | Number of Subjects | RPD, n (%) | OR (95% CI) | P Value a |
|---|---|---|---|---|
| Sex | .003 | |||
| Male | 27 | 5 (18.5) | 1 | |
| Female | 46 | 25 (54.4) | 5.2 (1.7–16) | |
| Categorical age (y) | .007 b | |||
| ≤80 | 25 | 6 (24.0) | 1 | |
| 81–86 | 20 | 7 (35.0) | 1.7 (0.46–6.2) | |
| ≥87 | 28 | 17 (60.7) | 4.9 (1.5–16) | |
| Categorical age at AMD onset (y) | .0003 b | |||
| ≤70 | 25 | 3 (12.0) | 1 | |
| 71–82 | 24 | 12 (50.0) | 7.3 (1.7–31.2) | |
| ≥83 | 24 | 15 (62.5) | 12 (2.8–53) | |
| Family member with AMD c | .3 | |||
| No | 53 | 19 (36.9) | 1 | |
| Yes | 19 | 10 (52.6) | 2.0 (0.69–5.7) | |
| Smoking (>6 months) | .6 | |||
| No | 30 | 11 (36.7) | 1 | |
| Yes | 43 | 19 (44.2) | 1.4 (0.53–3.6) | |
| Hypertension | .08 | |||
| No | 26 | 7 (26.9) | 1 | |
| Yes | 47 | 23 (48.9) | 2.6 (0.92–7.3) | |
| Hyperlipidemia | .5 | |||
| No | 35 | 16 (45.7) | 1 | |
| Yes | 38 | 14 (36.8) | 0.69 (0.27–1.8) | |
| Diabetes mellitus | .2 | |||
| No | 66 | 29 (43.9) | 1 | |
| Yes | 7 | 1 (14.3) | 0.21 (0.02–1.9) | |
| ARMS2 d risk allele (rs10490924) | .5 | |||
| −/− | 23 | 7 (30.4) | 1 | |
| +/− | 35 | 17 (48.6) | 2.2 (0.71–6.5) | |
| +/+ | 14 | 6 (42.9) | 1.7 (0.43–6.8) | |
| CFH e risk allele (rs1061170) | .6 | |||
| −/− | 10 | 5 (50.0) | 1 | |
| +/− | 45 | 17 (37.8) | 0.61 (0.15–2.4) | |
| +/+ | 17 | 8 (47.1) | 0.89 (0.19–4.2) |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


