3 Rhinology, Allergy, and Immunology
Overview
1 | What cells contribute to the formation of the nose during the 4th week of embryogenesis? | Neural crest cells |
2 | Before closure during embryogenesis, what are the following spaces called? • Between the frontal and nasal bones • Between the frontal and ethmoid bones • Between the nasal bones and nasal capsule | Fronticulus nasofrontalis Foramen cecum Prenasal space |
3 | What embryologic structures form within the thickened ectoderm of the nasal placodes of the frontonasal process and after dividing each placode into medial and lateral nasal processes become the early nasal cavities? | Nasal pits |
4 | Into what structures do the (1) medial and (2) lateral processes of the nasal pits and the (3) maxillary process of the maxilla develop? | • Medial: Nasal septum (from the globular processes of His), philtrum, premaxilla • Lateral: Nasal alae • Maxillary process: Lateral nasal wall |
5 | What embryologic membrane separates the nasal and oral cavities, and normally degenerates to allow open passages as the choanae are formed by the deepening olfactory pits during development? | Nasobuccal membrane |
6 | The nasal bones attach to what structures within the facial skeleton? | Frontal bone, nasal process of the maxilla, upper lateral cartilages, contralateral nasal bone, perpendicular plate of the ethmoid, and cartilaginous septum |
7 | What are the three different regions of the paired lower lateral cartilages of the nose? | • Medial crus • Intermediate crus • Lateral crus |
8 | What is the name of the area that connects the lower lateral cartilages with the upper lateral cartilages? | Scroll region |
9 | What are the boundaries of the internal nasal valve? ( | • Caudal septum • Head of the inferior turbinate • Remainder of tissues around the piriform aperture • Upper lateral cartilage, distal end Note: Also called the valve area, nasal valve region |

10 | What structure does the frontal process of the maxilla, nasal floor, and lateral fibrofatty tissue form? | Piriform aperture |
11 | What are the boundaries of the external nasal valve? | • Caudal septum • Lower lateral cartilage (caudal edge of the lateral crus, junction with the upper lateral cartilage) • Piriform aperture |
12 | Name the components of the nasal septum. ( | • Perpendicular plate of the ethmoid bone • Quadrangular cartilage • Vomer • Maxillary crest • Palatine bone |
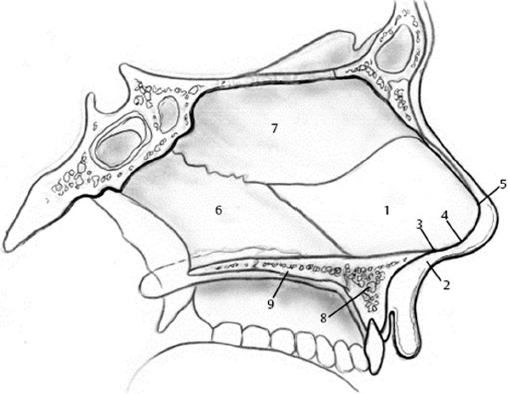
13 | What is the blood supply of the nasal septum? | • Anterior and posterior ethmoid arteries (superior septum) • Sphenopalatine artery branches/posterior septal branch (posterior/inferior septum) |
14 | Most cases of epistaxis arise in what area? | Kiesselbach plexus (Little area), anterior septum |
15 | The uncinate process is an extension of what bone? | Ethmoid bone |
16 | What are the three most common superior attachment points for the uncinate? ( | • Lamina papyracea • Skull base • Middle turbinate |
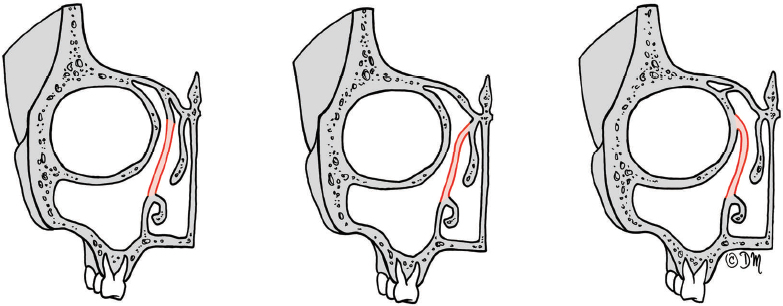
Fig. 3.3 The three most common superior attachment points of the uncinate process: (a) skull base; (b) middle turbinate; (c) lamina papyracea. (Used with permission from Levine HL, Clemente MP, eds. Sinus Surgery: Endoscopic and Microscopic Approaches. New York, NY: Thieme; 2005.)
How does the superior attachment of the uncinate process relate to the drainage of the frontal sinus outflow tract? | When attached to the lamina papyracea, the frontal sinus usually drains medial to the uncinate, and when it is attached to the skull base or middle turbinate, it often drains lateral to the uncinate. | |
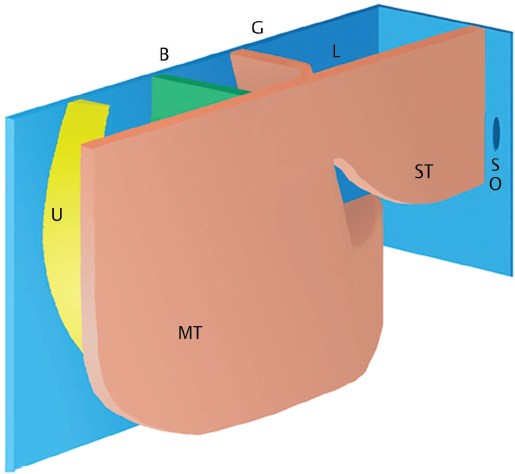
18 | What is the opening to the space between the uncinate process and the ethmoid bulla called? | Semilunar hiatus |
19 | The uncinate process covers the medial aspect of which space that provides a common drainage pathway for some of the anterior sinuses? | (Ethmoidal) Infundibulum |
20 | True or False. The uncinate attaches to the ethmoid crest of the maxilla, the lacrimal bone, the ethmoidal process of the inferior turbinate bone, and the palatine bone via the lamina perpendicularis. | True |
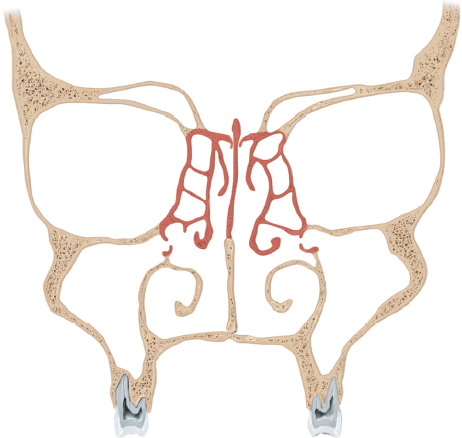
21 | The lamina papyracea is formed by which bone? | Ethmoid bone |
22 | The nasolacrimal duct empties under what structure in the nose? | Inferior turbinate (via the Hasner valve) |
23 | What is the name for a pneumatized middle turbinate, which is an extension of the ethmoid bone? | Concha bullosa |
24 | The middle turbinate attaches superiorly to the lateral aspect of the cribriform plate, laterally to the lamina papyracea/maxillary sinus, posteriorly to the lateral wall just anterior to the crista ethmoidalis of the palatine bone, and anteriorly near the agger nasi to what structure, which is a part of the frontal process of the maxilla? | Cristal ethmoidalis of the maxilla |
25 | What structure separates the anterior and posterior ethmoid sinuses? | Ground or basal lamella |
26 | What are the five ethmoturbinals, and what do they become? | First → Agger nasi (ascending portion) and uncinate process (descending portion) Second → Middle turbinate Third → Superior turbinate Fourth and fifth fuse → supreme turbinate |
27 | List the first four ethmoid lamellae. ( | • Uncinate process • Ethmoid bulla • Basal lamella of the middle turbinate • Lamella of the superior turbinate |
28 | What is the horizontal plate of the ethmoid bone that forms the roof of the ethmoid sinus and separates the ethmoid air cells from the anterior cranial fossa called? | Fovea ethmoidalis |
29 | What are the three infundibular cells that are anterior ethmoid air cells? | • Agger nasi cells • Terminal cell (recessus terminalis) • Suprainfundibular cell |
30 | Which cell type is the most anterior of the ethmoid cells and forms near the attachment of the middle turbinate to the lateral nasal wall? | Agger nasi cell(s) |
31 | After removing the uncinate process, the ethmoid bulla typically sets just anterior to the basal lamella. Where does this sinus drain? | Suprabullar or retrobullar recess (sinus lateralis) |
32 | What arterial structure typically runs through the roof of the ethmoid bulla? | Anterior ethmoid artery |
33 | The middle meatus, uncinate, infundibulum, anterior ethmoid cells, and ostia (frontal, ethmoid, maxillary) collectively are referred to as what? ( | Ostiomeatal complex |
34 | What is the name of the infraorbital ethmoid air cells that pneumatize into the maxillary sinus and can narrow the maxillary sinus ostium? | Haller cells |
35 | In the adult, the posterior ethmoidal complex consists of one to five cells, which typically drain into which space? | Superior or supreme meatus |
36 | Air cells that pneumatize lateral or posterior to the anterior wall of the sphenoid sinus are called what? | Onodi cells (sphenoethmoidal cell) |
37 | What is the first sinus to develop embryologically? | Maxillary sinus |
38 | What structure must be removed to visualize the natural ostium of the maxillary sinus? | Uncinate process |
39 | Where is the most common location for the maxillary ostium within the infundibulum? | Inferior third (65%) |
40 | Where are the anterior and posterior nasal fontanelles located? | Located anterior and posterior to the inferior aspect of the uncinate process |
41 | What structure runs through the roof of the maxillary sinus? | Infraorbital nerve |
42 | A series of three or four frontal furrows arise out of the ventral middle meatus and give rise to what? | • First frontal furrow = agger nasi cell • Second frontal furrow = frontal sinus • Third and fourth furrow = anterior ethmoid cells |
43 | What is the last sinus to fully develop, and at what age has it typically reached full size? | Frontal sinus. Late teens |
44 | The frontal sinus drains via the frontal sinus outflow tract or frontal recess into which space? | Ethmoid infundibulum (most common) |
The frontal or frontoethmoidal cells are located superior to the agger nasi cell and can have quite variable pneumatization. Describe the four Kuhn types of pneumatization. | • Type I: Single cell superior to the agger nasi but not extending into the frontal sinus • Type II: Tier of two or more cells above the agger nasi but below the orbital roof • Type III: Single cell extending from the agger nasi into the frontal sinus • Type IV: Isolated cell within the frontal sinus | |
46 | What type of cell can be found posterior to the frontal sinus and superior to the orbit? ( | Supraorbital ethmoid cells |
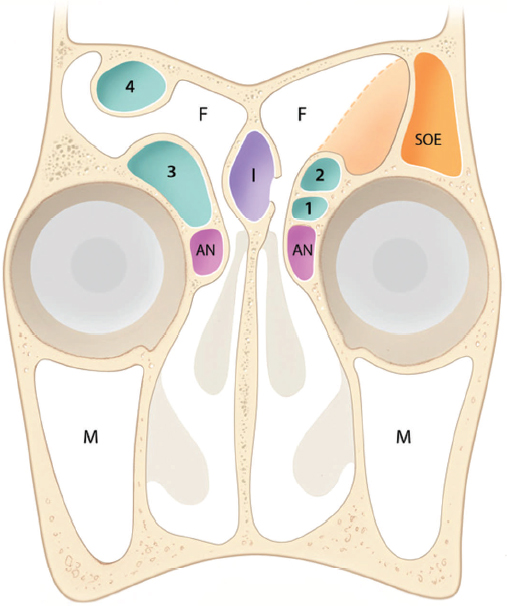
Fig. 3.6 Anatomic variations of the frontal sinus and frontal recess. M, maxillary sinus; F, frontal sinus; AN, agger nasi cell; 1–4, type 1–4 frontal cells; SOE, supraorbital ethmoid cell; I, frontal intersinus septal cell. (Used with permission from Kennedy DW, Hwang PH, eds. Rhinology: Diseases of the Nose, Sinuses, and Skull Base. New York, NY: Thieme; 2012.)
47 | The spread of frontal sinus infections intracranially is commonly thought to pass through what structures? | Foramina of Breschet (small venules that drain the frontal sinus mucosa to the dural veins) |
48 | How is the sphenoid sinus formed during development? | Nasal mucosa invaginates into the cartilaginous nasal capsule, which forms the cupolar recess. The wall of this recess becomes ossified later in development into the ossiculum Bertini. The cartilage is resorbed in the 2nd and 3rd years of life, and the ossiculum attaches to the sphenoid bone. Pneumatization then progresses and is complete in the 9th to the 12th years. |
What is the most posterior paranasal sinus, and where does its natural ostium drain? | Sphenoid sinus; sphenoethmoidal recess (between the superior turbinate and the anterior wall of the sphenoid sinus) | |
50 | Describe four surgical landmarks to help safely identify the natural ostium of the sphenoid sinus. | • 6.2 to 8.0 cm from the anterior nasal spine • 30 to 40 degrees from the nasal floor • Medial to the posterior end of the superior turbinate (85%) • ~ Halfway up the anterior sphenoid wall |
51 | The carotid artery is reported to be dehiscent in the sphenoid sinus in what percent of patients? | ~ 15% |
52 | What are the main types of sphenoid pneumatization in the Hamberger classification? | • Conchal type: No pneumatization • Presellar type: Pneumatization restricted anterior to a vertical plane passing through the anterior clinoid process • Sellar type: Well-pneumatized, most common (90%); can be complete or incomplete depending on whether the pneumatization extends to the clivus |
53 | When removing the intersinus septum within a sphenoid sinus, attachment of this septation to what critical structure must be considered? ( | Internal carotid artery |
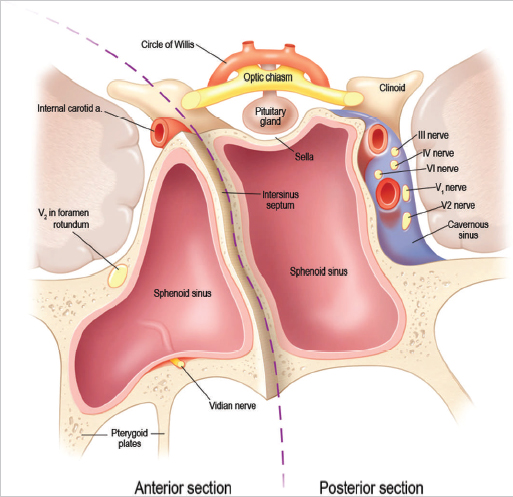
Fig. 3.7 Oblique view of the sphenoid sinus. Dashed line demonstrates the proximity of the intersinus septum to the internal carotid artery. Also note that cranial nerve 6 is the most medial cranial nerve in the cavernous sinus explaining why abducens palsy may be preferentially affected in sphenoid disease. (Used with permission from Kennedy DW, Hwang PH, eds. Rhinology: Diseases of the Nose, Sinuses, and Skull Base. New York, NY: Thieme; 2012.)
54 | What is the space between the internal carotid artery and the optic nerve within the sphenoid sinus called? | Opticocarotid recess |
55 | What portion of the internal carotid artery can be seen within the sphenoid sinus? (Inter) cavernous portion: | • Presellar: Anterior vertical segment and anterior bend • Infrasellar: Short horizontal segment • Retrosellar: Posterior bend and posterior vertical segment |
What neurovascular structures set within the parasellar cavernous sinus? | • Internal carotid artery • Cranial nerves III, IV, and VI • Cranial nerves V1 and V2 | |
57 | What anatomical structures pass through the optic canal? | • Optic nerve • Ophthalmic artery • Ophthalmic vein |
58 | The vidian nerve is formed by which two nerves before it runs through the vidian canal and exits into the pterygopalatine fossa? ( | • Greater superficial petrosal nerve from the geniculate ganglion of the facial nerve (parasympathetic fibers from the superior salivary nucleus) • Deep petrosal nerve from the sympathetic plexus of the internal carotid artery (sympathetic fibers) |
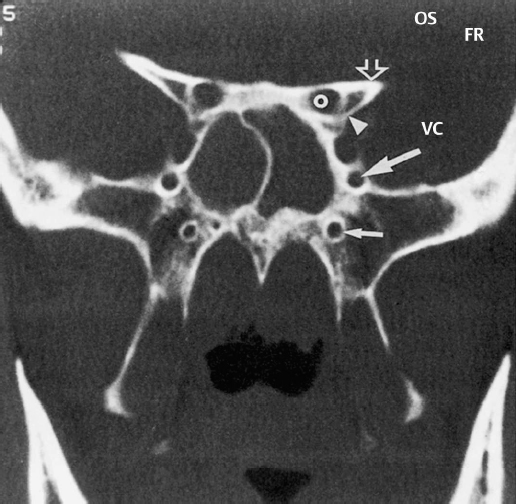
Fig. 3.8 Coronal CT scan at the sphenoid sinus and pterygoid plates. The vidian canal (VC), foramen rotundum (FR), optic strut (OS), and optic canal (O) can be seen. (Used with permission from Mafee MF, Valvassori GE, Becker M. Imaging of the Head and Neck 2nd Edition. New York, NY: Thieme; 2005.)
59 | What is the lateral craniopharyngeal canal that may persist in the adult patient anad lead to encephalocele formation and cerebrospinal fluid (CSF) leak and most commonly is noted in patients with significant lateral pneumatization of the sphenoid sinus? | Sternberg canal |
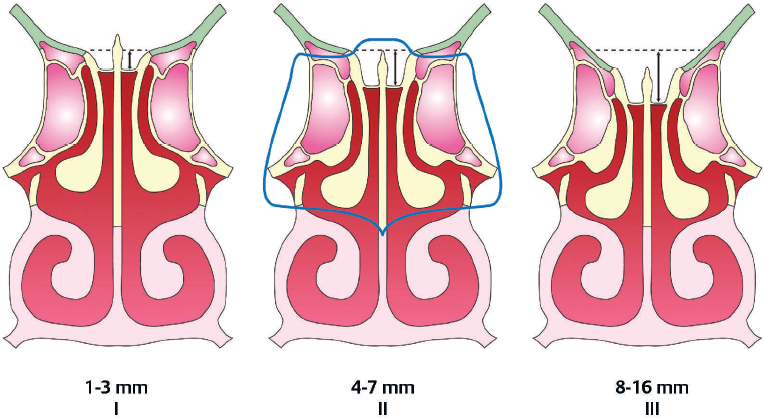
60 | The cribriform plate lies medially within the anterior skull base, surrounded laterally by what structure? | Fovea ethmoidalis (roof of the ethmoid sinuses): Joins the cribriform plate via the lateral lamella of the cribriform plate, which is often quite thin |
61 | According to Keros et al (Laryngol Rhinol Otol, 1965), the anterior skull base can be described based on the depth of the cribriform plate in relation to the fovea ethmoidalis according to which three classifications? ( | • Type I: 1 to 3 mm • Type II: 4 to 7 mm • Type III: 8 to 16 mm (highest risk for iatrogenic injury) |
62 | Describe the slope of the anterior skull base from anterior to posterior. | Highest anteriorly, lowest posteriorly |
63 | What major branches of the internal maxillary artery provide arterial blood supply to the nose? | • Sphenopalatine artery • Descending palatine artery → greater and lesser palatine arteries |
64 | The sphenopalatine foramen is located posterior to the attachment of the middle turbinate to the lateral nasal wall, may have several foramina, and almost always is demarcated by what small, raised, bony crest just anterior or anteroinferior to the foramen? | Crista ethmoidalis of the palatine bone |
65 | The sphenopalatine artery can exit the foramen in up to 10 separate branches, what are the most common branches and their distribution? | • Lateral nasal artery: Lateral nasal wall including the turbinates • Posterior septal artery: Posterior/inferior septum |
66 | When ligating the anterior ethmoid artery via an external approach, the vessel can be found running in what suture line? | Frontoethmoid suture |
67 | What is the distance between the anterior lacrimal crest of the maxilla’s frontal process to the anterior ethmoid artery? | 20 to 25 mm |
68 | What is the average distance between the anterior and posterior ethmoid arteries? | 10 to 19 mm |
69 | What is the average distance from the posterior ethmoid artery to the optic nerve? | 3 to 7 mm |
70 | What intranasal vessels are branches of the internal carotid artery? | Anterior and posterior ethmoid arteries |
What is the blood supply to the nasal septum? | • Superior labial artery (anteriorly) • Greater palatine artery (posteriorly) • Anterior and posterior ethmoid arteries (superiorly) • Posterior septal artery (posterior and inferiorly) | |
72 | What arterial plexus is formed along the posterior lateral nasal wall just under the inferior turbinate by branches from the ascending pharyngeal, posterior ethmoid, sphenopalatine, and lateral nasal arteries? | Woodruff plexus |
73 | True or False. Venules within the respiratory mucosa of the nasal and paranasal cavities do not have valves. | True |
74 | Where do the (1) sphenopalatine, (2) ethmoid, (3) angular, and (4) anterior facial veins drain? | • Pterygoid plexus • Superior ophthalmic vein • Ophthalmic vein → cavernous sinus • Common facial vein → internal jugular vein |
75 | What is the primary blood supply to the external nose? | • Angular artery (facial artery) • Superior labial artery (facial artery) |
76 | What arterial supply contributes to the formation of the Kiesselbach plexus (the Little area)? | • Posterior septal artery (sphenopalatine artery, external carotid artery) • Anterior ethmoid artery (ophthalmic artery, internal carotid artery) • Greater palatine artery (internal maxillary artery, external carotid artery) • Septal branches of the superior labial artery (facial artery, external carotid artery) |
77 | What major nerve branches arise from the nasociliary nerve (V1), and what regions of the nose do they supply? | • Infratrochlear nerve → medial eyelid skin • Anterior ethmoid nerve → anterior/superior nasal cavity, lateral nasal wall, and septum, external skin of nasal tip |
78 | After exiting the foramen rotundum, the maxillary nerve (V2) contributes fibers to the pterygopalatine (sphenopalatine) ganglion, which then supplies innervation to the nose via which branches? | • Infraorbital nerve → anterior area of inferior meatus, anterior nasal floor, nasal vestibule • Superior nasal branches (medial/lateral posterior) → posterior superior/middle turbinates, posterior ethmoid sinuses, face of the sphenoid, nasal vault, posterior septum • Nasopalatine nerve → anterior hard palate • Greater palatine nerve → middle/inferior meatus, posterior aspect of inferior turbinate |
79 | Where do the parasympathetic fibers that provide vasodilation and secretomotor stimulation to mucous glands synapse? | • Pterygopalatine (sphenopalatine) ganglion • Superior salivatory nucleus → nervus intermedius → geniculate ganglion → vidian nerve → pterygopalatine ganglion → sphenopalatine nerve branches → vasodilation/secretomotor function |
80 | Postganglionic sympathetic fibers that ultimately control vasoconstriction in the nose arise from what ganglion? | • Superior cervical ganglion • T1–T3 → superior cervical ganglion → internal carotid artery plexus → join greater superficial petrosal nerve → vidian nerve → pterygopalatine ganglion → sphenopalatine nerve branches → vasoconstriction |
81 | Where do olfactory neurons synapse? | • Olfactory bulb • Olfactory receptor neurons → unmyelinated axons → myelinated fascicles → olfactory fila/cribriform plate/→ olfactory bulb → olfactory tract |
Name the bones of the orbit. ( | • Lacrimal bone • Ethmoid bone • Frontal bone • Maxillary bone • Sphenoid bone • Zygomatic bone • Palatine bone |

Fig. 3.10 Bones of the orbit: lacrimal, ethmoid, frontal, maxillary, sphenoid, zygomatic, palatine. (Used with permission from Thieme Atlas of Anatomy: Head and Neuroanatomy, © Thieme 2007, illustration by Karl Wesker.)
83 | What extraocular muscle is at highest risk during medial orbital decompression for Graves ophthalmopathy? | Medial rectus muscle |
84 | What epithelium covers the cribriform plate bilaterally, extending to the superior and middle turbinates? | Olfactory neurepithelium: Pseudostratified columnar epithelium containing bipolar spindle-shaped olfactory receptor cells (cranial nerves I and V), columnar sustentacular cells, microvillar cells, and basal cells. Note: This sets on a vascular lamina propria containing Bowman (olfactory) glands and no submucosa. |
85 | What part of the nasal cavity is composed of stratified keratinizing squamous epithelium, hair follicles, sebaceous glands, and sweat glands? | Nasal vestibule |
86 | What ectodermally derived epithelium lines most of the nasal and paranasal cavities? | Ciliated pseudostratified columnar (respiratory) epithelium with ciliated and nonciliated columnar cells, mucoserous (minor salivary) glands within the submucosa, goblet cells, and basal cells Note: Anterior third → squamous and transitional cell epithelium, posterior two-thirds → pseudostratified columnar epithelium |
Ciliated columnar cells may contain 50 to 200 cilia per cell with each cilia arranged in a specific pattern. On electron microscopy, what do you expect to see for a normal ciliary structure? | “9 + 2” microtubules in doublets (dynein arms) | |
88 | What is another name for the ciliated pseudostratified columnar epithelium that lines the nasal and paranasal cavities? | Schneiderian membrane (ectodermally derived) |
89 | In normal individuals, the mucosa of one nasal passageway will be congested compared with the contralateral side owing to cyclic engorgement of the nasal turbinates. What is this normal physiologic phenomenon, which may function to optimize humidification and warming of the air, called? | Nasal cycle |
90 | What is the length of the average nasal cycle? What factors can cause an increase or decrease in “congestion” on a given side? | • Average cycle: 2 to 4 hours • Decreased exercise, increased heart rate • Increased: on “down” side when lying on one’s side |
91 | True or False. The nasal mucosal microvasculature is under parasympathetic tone. | False. Sympathetic tone → vasoconstriction → when tone decreases → increased vasodilation. Changes in tone result in the normal nasal cycle. |
92 | What is typically the narrowest area inside the nose, which creates the area of greatest resistance to airflow? | Internal nasal valve |
93 | Without changing nasal resistance, injecting lidocaine into the nose can result in the sensation of nasal obstruction, whereas inhaling menthol, camphor or eucalyptol can result in the sensation of a more “open” nasal passageway. Why? | Change in the level of activity of cold receptors, located predominantly in the nasal vestibule |
94 | On what is airflow through the nose dependent? | • Cross-sectional area of the nasal passageway • Pressure differential across the nose • Laminar vs. turbulent airflow |
95 | Describe the Bernoulli principle with respect to the nasal valve. | The speed of a fluid through a tubular structure is greatest at the point of smallest diameter. At the point of maximum velocity, the pressure reaches a nadir. The difference between intranasal pressure at the nasal valve and atmospheric pressure leads to potential for collapse. |
96 | As air moves from the nasal vestibule to the nasopharynx, the relative humidity increases by approximately what percent? | 95% |
97 | What nasal structure filters out large particles (20 to 30 μm) from the air? | Nasal vibrissae • Nasal septum and turbinates filter particles 10 to 30 μm. • Bronchial tree mucosa filters out particles 2 μm in diameter. • Particles 0.2 to 0.5 μm in diameter tend to remain suspended and are exhaled. |
98 | The nose filters out particles from the air larger than what size? Particles smaller than this size are able to reach the alveoli of the lungs. | 5 μm |
99 | What are the two mucous layers associated with the nasal mucociliary system? ( | • Upper gel layer: Trap inhaled particle; formed by goblet cells and submucosal glands • Lower sol layer; surround cilia of epithelium; formed by microvilli |
100 | What cells are responsible for producing the airway mucus? | • Goblet cells: Secrete mucins • Submucosal Seromucous glands: secrete mucins • Epithelial cells: Hydration of the mucus via active transepithelial transport systems • Venules: Plasma proteins |
101 | What factors can contribute to decreased mucociliary clearance? | • Dysfunction of cilia: Trauma, environmental damage, genetic disorder (i.e., primary ciliary dyskinesia, Kartagener syndrome, cystic fibrosis, etc.) • Altered mucus production or viscosity: Cystic fibrosis |
102 | What test can be used to measure mucociliary transport time in the nose? | Saccharin test: A saccharin pellet is placed in the anterior nasal cavity and dissolves, passing toward the oropharynx via the mucociliary system and resulting in the sensation of a sweet taste. Time for placement to sensation: < 20 minutes. |
103 | What nasal reflex results in congestion/swelling of the nasal mucosa when lying in a dependent position? | Postural reflex |
104 | Which nerves contribute to the overall experience of an odor? | • Olfactory nerve • Trigeminal nerve • Vagus nerve • Glossopharyngeal nerve |
105 | What produces the nasal mucus, a key component of olfaction? | Bowman glands found within the lamina propria beneath the olfactory epithelium and goblet cells and submucous glands found within the adjacent respiratory epithelium produce mucus |
106 | What type of cell is responsible for olfaction? | Olfactory receptor cells are bipolar ciliated neurons. |
What layer(s) must odorants penetrate to reach the olfactory receptor neurons? | Olfactory mucus | |
108 | What organ is often noted in the anteroinferior nasal septum as a small pit whose function in humans is unknown but in many other mammals is thought to be related to the detection of pheromones? | Vomeronasal organ (Jacobson organ) |
109 | What characteristics of particles are important for their recognition by the olfactory nerves? | For particles to be recognized by the olfactory nerves, the particles must be volatile substances that are lipid soluble. |
110 | What terms are associated with each of the following? • Normal olfaction • Complete loss of smell • Decreased sense of smell • Altered perception of smell • Perception of odor without stimulus present • Altered perception of an odor in the presence of an odorant stimulus | • Normosmia • Anosmia • Hyposmia • Dysosmia • Phantosmia • Parosmia or troposmia |
111 | Describe the two main types of olfactory dysfunction. | • Conductive olfactory loss: Occurs secondary to obstruction of the nasal airflow to the olfactory cleft • Sensorineural or nonconductive olfactory loss: Occurs secondary to damage or dysfunction of the olfactory neurons anywhere along the olfactory system |
112 | What are common causes of conductive olfactory loss? | • Chronic rhinosinusitis (CRS), allergic rhinitis, polyps, septal deflection, tumors • Also occurs with diverted airway (tracheostomy or laryngectomy) from diminished or absent airflow through the nose |
113 | What are common causes of sensorineural olfactory loss? | Post-upper respiratory tract infection (UTI; viral) loss, CRS (certain patients), head trauma, toxin exposure, congenital disorders, dementia, Alzheimer disease, Parkinson disease, multiple sclerosis |
114 | How often does olfactory loss occur after head trauma, and when does it occur? | 5% to 10% The amount of loss usually correlates with the severity of trauma. Onset is often immediate but can be delayed for months. |
115 | What is the mechanism thought to be associated with olfactory dysfunction resulting from head trauma? | Shearing of the olfactory nerve axons, contusion/hemorrhage within the olfactory regions of the brain, or structural alteration of the sinonasal tract The most common trauma type is impact to the frontal region, followed by trauma to the occiput. |
116 | How does post-traumatic olfactory dysfunction differ in the pediatric population compared with that in adults? | Olfactory dysfunction is less common: 3.2% transient dysfunction and 1.2% with permanent dysfunction. |
117 | What percentage of adults will recover their sense of smell after experiencing anosmia from a head trauma? | 5 to 10% |
118 | What is the most common cause of olfactory loss? | Persistent olfactory dysfunction after URI. This type of olfactory loss is more common in women, typically women older than 50 years (70 to 80% of cases). |
119 | What proportion of patients will likely recover their sense of smell following a postviral URI, regardless of treatment? | ~ One-third |
Olfaction is dependent on the health of the olfactory neural elements, which are slowly lost over time, resulting in an age-dependent decline in olfaction, most noticeable after what decade(s)? | Sixth and seventh | |
121 | Olfactory function can be lost after exposure to specific toxins, such as formalin or cigarette smoke. What factors most strongly influence the olfactory dysfunction? | • Type of toxin • Concentration and duration of exposure |
122 | In what two neurologic diseases is olfactory loss thought to be one of the earliest signs? | Parkinson disease and Alzheimer disease |
123 | What disorder is associated with anosmia and hypogonadism? | Kallmann syndrome (hypogonadotropic hypogonadism); can be X-linked (KAL 1 gene) or autosomal dominant (KAL 2 gene) |
124 | Describe Kallmann syndrome and its relation to congenital olfactory dysfunction. | Gonadotropin-releasing hormone neurons fail to migrate from the olfactory placode to the hypothalamus. Magnetic resonance imaging (MRI) may demonstrate the absence of olfactory bulbs. |
125 | In what familial autosomal dominant condition do patients develop anosmia, early baldness, and bilateral vascular headaches? | Familial anosmia |
126 | What advice is critical to relay to patients with significantly impaired olfaction? | It is critical to review the risks of inability to smell “warning” odors, such as smoke, natural gas, and spoiled foods, and to recommend the use of smoke alarms and natural gas detectors. |
127 | Describe the principle of olfactory threshold testing and one method of performing it. | Absolute threshold of detection is identified, which is the lowest concentration of an odorant that can be detected reliably. An odorant in one sniff bottle and water in another bottle are presented at varying concentrations from weak to strong (based on distance). |
128 | Describe the principle of odor identification tests. | This is a quantitative test (number of odorants identified). Odorants are presented at suprathreshold concentrations to a patient who is asked to identify the odorants. |
129 | Describe the University of Pennsylvania Identification Test (UPSIT). | The UPSIT is a self-administered test with four “scratch and sniff” booklets, each containing 10 odorants. Each odorant has a question with four answers. The patient is required to answer even if he or she does not recognize the odorant. Random-chance performance would be 10 of 40, so scores lower than 5 are concerning for malingering. The UPSIT has been studied extensively, and the reliability of the test is high. |
130 | Describe the Cross-Cultural Smell Identification Test (CC-SIT). | This test is a variant of the UPSIT. It comprises 12 items (banana, chocolate, cinnamon, gasoline, lemon, onion, paint thinner, pineapple, soap, smoke, and turpentine) and is based on odorants most consistently identified by subjects representing various countries (China, France, Germany, Italy, Japan, Russia, and Sweden). |
131 | What are the most common side effects of second-generation histamine type 1 (H1) blockers? | Headache, urinary retention, dry mouth, blurry vision, and GI upset |
132 | What is the most common side effect of intranasal steroid sprays? | Epistaxis resulting from incorrect technique |
133 | What are the most common side effects of pseudoephedrine? | Nervousness, hypertension, and urinary retention |
134 | What is the onset of action of cocaine? | 5 to 10 minutes |
What is the duration of action of cocaine? | 6 hours | |
136 | What is the maximum recommended dose of cocaine? | Varies between 1 and 3 mg/kg; 3 mg/kg is most common. Commonly comes in a 4% solution, and it is estimated that < 40% is truly absorbed. |
Disorders of the Nasal Valve and Septum
137 | What are the two general forms of nasal valve obstruction? | • Static = does not change with respiration (i.e. caudal septal deviation) • Dynamic = changes with respiration, causes collapse of the structures of the nasal valve (i.e. internal nasal valve collapse) |
138 | While examining a patient, you use lateral distraction on the cheek while asking the patient to breathe in and out and tell you whether this maneuver increases airflow. What is the name of this test, and what is it most useful for? | Cottle maneuver. Nonspecific. Almost all nasal obstruction improves with this maneuver. It can point to internal nasal valve collapse, which can also be demonstrated with Breathe Right strips. |
139 | How does the modified Cottle maneuver differ from the Cottle maneuver? | The modified Cottle maneuver is performed by placing an ear curette or end of a Q-tip inside the nose with gentle support of the internal and/or the external nasal valve while the patient breathes to determine whether his or her breathing improves. The modified test is a better test than the Cottle maneuver. |
140 | What test can be used to determine whether the inferior turbinates are a significant contributor of nasal airway obstruction? | Spray the patient’s nasal cavities with phenylephrine spray to decongest the patient’s inferior turbinates and determine whether nasal obstruction improves. |
141 | What is the point of highest resistance in the adult airway? | Internal nasal valve |
142 | What structure visualized on anterior rhinoscopy is responsible for two-thirds of upper airway resistance at the internal nasal valve? | Inferior turbinate |
143 | On anterior rhinoscopy you note a normal, but enlarged, middle turbinate. On CT scan, there is an air-filled sinus within the head of the middle turbinate. What is the most likely cause? | Concha bullosa: Pneumatized middle turbinate |
144 | What percentage of the population will have a concha bullosa? | 25% |
145 | What is the approximate angle between the septum and upper lateral cartilage within the internal nasal valve? | 10 to 15 degrees |
146 | Identify treatment options for both internal and external nasal valve collapse. | Septoplasty, batten grafts, spreader grafts, lateral crural strut grafts, lower lateral cartilage suture suspension |
147 | List the possible causes of nasal septal perforation. | • Iatrogenic: Prior septal surgery, prior cauterization, nasogastric tube placement, nasotracheal intubation, etc. • Trauma: Nose picking (i.e., digital trauma), septal hematoma • Inhalants: Cocaine abuse, intranasal corticosteroids, chronic vasoconstrictor use, glass dust, etc. • Autoimmune: Wegener granulomatosis, sarcoidosis, systemic lupus erythematosus, Crohn disease, etc. • Infectious: Syphilis, leishmaniasis, tuberculosis, acquired immunodeficiency syndrome (AIDS), etc. • Neoplastic: T-cell lymphomas, etc. • Miscellaneous: Lime dust, cryoglobulinemia, renal failure • Idiopathic |
What common symptoms are associated with septal perforation? | • Asymptomatic (vast majority) • Nasal crusting • Epistaxis • Nasal obstruction • Postnasal drip • Whistling | |
149 | Where are septal perforations most commonly found in the septum, and how large are they usually? | Anterior septum. Most commonly 1 to 2 cm |
150 | When should you take a biopsy of a septal perforation? | When there is concern for malignancy, a biopsy should be taken, although this is controversial and not recommended routinely; yield is low when biopsy is done for vasculitic disease, etc. |
151 | What size septal perforation has a high risk of failed surgical closure? | Large perforation (> 2 cm) |
152 | What perforations should you treat with conservative management, and what does this involve? | Asymptomatic perforations. The goal is to keep the perforation moist (i.e., nasal saline sprays, Vaseline, saline irrigations, etc.). |
153 | For large septal perforations not amenable to surgical closure or smaller symptomatic perforations, what nonsurgical option can be offered that can decrease epistaxis, nasal crusting, obstruction, and whistling? | Septal button placement. Prefabricated or custom buttons are available. Custom prostheses for large or irregular perforations can be optimally sized using a maxillofacial CT scan. |
154 | Identify complications associated with septal button placement. | • Intranasal pain (particularly if displaced) • Erosion of perforation edges (rare, usually protects) • Intranasal crusting • Bacterial colonization/biofilm Note: All are relatively low risk but should be discussed. |
155 | Describe the surgical approaches and techniques available for nasal septal perforation repair. | Approaches: Endonasal versus open techniques: • Primary closure • Interposition grafts: Bone, cartilage, periosteum, temporalis fascia, acellular dermis • Flaps: Bipedicaled mucoperichondrial flap, rotational mucoperichondrial flap • Alternative flaps (large perforations > 2 cm): Inferior turbinate pedicled flap, tunneled sublabial mucosal flap, facial artery musculomucosal flap, radial forearm free flap, pericranial/glabellar flap |
156 | Describe the process and potential danger of septal hematoma. | Blood collection causes elevation of the mucoperichondrium/mucoperiosteum off the septal cartilage causing devascularization of underlying cartilage and potential for avascular necrosis and reabsorption. |
157 | Identify complications associated with septal hematoma. | Septal perforation, subperichondrial fibrosis, septal abscess, intracranial infection (spread to cavernous sinus through emissary veins, extremely rare) |
158 | What factor places children at increased risk for developing nasal septal hematoma? | Loose adherence of the mucoperichondrium and mucoperiosteum to the underlying bone and cartilage |
159 | What is the treatment for septal hematoma? | Incision and drainage with application of nasal stent or packing to keep the potential space reduced. The patient should be receiving prophylactic antibiotics while packing is in place. |
What is defined as a collection of purulent material between the nasal septal mucoperiosteum/mucoperichondrium and the bony and/or cartilaginous septum? | Nasal septal abscess | |
161 | What are the risk factors for developing a nasal septal abscess? | • Septal hematoma resulting from trauma or prior surgery • Nasal vestibule furuncle • Sinusitis • Dental infection |
162 | What is the recommended management for nasal septal abscesses? | • Anti-staphylococal antibiotics • Incision and drainage |
163 | What complications are associated with nasal septal abscesses? | Intracranial complications (abscess, cavernous sinus thrombosis), orbital cellulitis, septal perforation or weakening or loss of the nasal framework resulting in saddle-nose deformity |
164 | A patient with pain and itching of the nasal vestibule is examined, and you note small pustular lesions with an erythematous base, pierced by a single hair follicle. What is the diagnosis? | Nasal folliculitis |
165 | Facial or nasal folliculitis can be superficial or deep and is often associated with what pathogen? | S. aureus |
166 | What pathologic condition generally follows folliculitis, or hair follicle infection, and develops as a small abscess with extension of purulent material from the dermis to subcutaneous tissue? | Furuncle (boil) |
167 | Why are incision and drainage of nasal furuncles, if necessary, deferred for at least 24 hours after initiating antistaphylococcal antibiotics? | Risk of cavernous sinus thrombosis |
168 | Inflammatory nasal masses can form around a foreign body, blood clot, or secretion and grow as a result of accumulation of salts (calcium, magnesium, phosphate, carbonate) over time, potentially resulting in pressure injury to adjacent structures and causing nasal obstruction, pain, headache, infection, or recurrent epistaxis. This process is referred to as what? | Rhinolith |
169 | A previously healthy 3-year-old patient has had 2 days of unilateral rhinorrhea associated with a foul odor, intermittent ipsilateral epistaxis, and generalized irritability. Examination reveals a mass in the right nasal cavity. What is the most likely diagnosis? | Nasal foreign body |
170 | What proportion of epistaxis arises from an anterior source? | Approximately 90% to 95% |
171 | What are the common local causes of epistaxis? | • Trauma: Digital, fracture, nasotracheal intubation, feeding tube placement, foreign body, recent surgery • Drug related: Nasal steroid sprays, cocaine inhalation • Desiccation: Nasal oxygen, continuous positive airway pressure (CPAP) • Inflammatory or infectious • Neoplastic |
172 | What systemic processes can result in epistaxis? | Coagulopathy: • Genetic: Hemophilia, hereditary hemorrhagic telangiectasis (HHT), von Willebrand disease • Drug related: Coumadin, heparin, aspirin • Hypertension • Neoplastic: Pancytopenia, thrombocytopenia, etc. |
List nonsurgical methods of epistaxis management. | ABCs (airway, breathing, and circulation): Epistaxis can be life threatening! • Direct pressure • Vasoconstrictive agents • Cautery under direct visualization • Nasal packing • Absorbable packing • Nonabsorbable packing • Control hypertension and correct coagulopathy if possible • Nasal hygiene • Saline sprays, humidity, emollients (petroleum jelly, etc.) | |
174 | What are the surgical methods available for epistaxis control if bleeding continues despite maximum nonoperative intervention? | • Surgical ligation • Sphenopalatine artery (transnasal endoscopic, identify crista ethmoidalis, may use large maxillary antrostomy) • Internal maxillary artery (transmaxillary endoscopic, either via the Caldwell-Luc procedure, mega-antrostomy, or partial medial maxillectomy) • Anterior ethmoid artery (Lynch incision, identify frontoethmoid suture line) • External carotid artery (transcervical) • Endovascular embolization (most commonly internal maxillary artery; risk of stroke) |
175 | External ligation of the anterior ethmoid artery is obtained through what approach? | Accessed via Lynch incision, located approximately 24 mm posterior to the anterior lacrimal crest, along the frontoethmoid suture line |
176 | Describe the location of the sphenopalatine artery for endoscopic ligation. | Posterior to the inferior attachment of the middle turbinate, submucosal on the lateral nasal sidewall |
177 | Why are antibiotics prescribed while a patient has nasal packing in place? | To prevent toxic shock syndrome |
178 | What autosomal dominant disorder results in punctate hemangiomas or vascular sinuses that are irregularly shaped, associated with thin epithelium, and have no muscular or elastic layers resulting in easy bleeding? | Osler-Weber-Rendu disease (HHT) |
179 | What are the organs most commonly associated with HHT? | Nasal cavity, oral cavity, GI tract, lungs, liver |
180 | Which genetic mutations are most commonly seen with HHT? | Endoglin gene (ENG, HHT1) and activin A receptor type II-like 1 gene (ACVRL1, HHT2). Mutation detection rates are as high as 75% with sequence analysis of these two genes. SMAD4 is less common (3%) and is associated with HHT and juvenile intestinal polyposis. |
181 | What are the most common sign and symptom associated with HHT? | Mucocutaneous telangiectasias and recurrent epistaxis |
182 | What are the nonsurgical treatment options available for HHT patients with recurrent epistaxis? | • Anemia: Iron supplementation, blood transfusions • Nasal hygiene: Oil of sesame with rose-geranium, nasal saline spray; tolerated in some patients • Intranasal bevacizumab |
183 | What are the surgical treatment options available for HHT patients with recurrent epistaxis? | Surgical management: • Potassium-titanyl-phosphate (KTP) laser ablation of lesions • Injection of bevacizumab • Septodermoplasty • Young’s procedure |
Describe Saunder’s septodermoplasty. | Denuding of nasal mucosa affected by telangiectasias and coverage of denuded area with a split-thickness skin grafts | |
185 | In what surgical procedure are the nasal cavities closed by creating two layered flaps (nasal mucosa and skin), thus eliminating airflow through the nasal cavities? | Young’s procedure |
Rhinitis
186 | A patient with irritation and inflammation of the nasal mucous membranes complains of rhinorrhea, nasal congestion, and postnasal drip. What is the most likely general diagnosis based on this information? | Rhinitis |
187 | What are the main forms of rhinitis? | • Allergic rhinitis • Nonallergic rhinitis |
188 | Allergic rhinitis reflects what type of Gell and Coombs hypersensitivity? | Type I (anaphylactic/immediate) hypersensitivity with both early and late-phase reactions occurring after re-exposure to the antigen (see section on Allergy) |
189 | What are the primary subtypes of allergic rhinitis? | • Seasonal allergic rhinitis • Perennial allergic rhinitis • Mixed allergic rhinitis |
190 | What are the classic symptoms of allergic rhinitis? | • Sneezing • Rhinorrhea • Nasal congestion • Pruritus (nasal, palatal, ocular) • Watery eyes • Postnasal drainage • Anosmia/hyposmia |
191 | Diagnosis of allergic rhinitis hinges most heavily on what factor? | Clinical history |
192 | What comorbidities are commonly associated with allergic rhinitis? | Asthma, acute rhinosinusitis, otitis media with effusion, sleep disordered breathing, and obstructive sleep apnea |
193 | What treatments exist for allergic rhinitis? | Intranasal/oral corticosteroids, intranasal/oral antihistamines, leukotriene inhibitors, cromolyn sodium, immune therapy (sublingual and injection) (see section on Allergy) |
194 | A patient presents with nasal congestion, rhinorrhea, and postnasal drip but has a history of negative allergy testing. What type of rhinitis does this most likely represent? What are the major subtypes associated with this condition? | • Nonallergic rhinitis:
|
195 | What are the key symptoms associated with non-allergic rhinitis? | • Sneezing • Rhinorrhea • Nasal congestion • Postnasal drainage |
196 | True or False. Negative allergy testing is required for the diagnosis of nonallergic rhinitis. | False |
Viral infections (rhinovirus, respiratory syncytial virus, parainfluenza virus, adenovirus, influenza virus, and enterovirus) can result in URI symptoms, including congestion, rhinorrhea, and postnasal drip, but often they do not cause pruritic symptoms. The infection typically resolves within 7 to 10 days. What diagnosis does this describe? | Infectious rhinitis | |
198 | In what type of nonallergic rhinitis is there excess parasympathetic tone resulting in vasodilation, which can be triggered by cold temperatures and strong smells? | Vasomotor rhinitis |
199 | What are the characteristics of vasomotor rhinitis? | It is a diagnosis of exclusion. Patients usually manifest this condition in older age, with copious clear rhinorrhea that is triggered by alcohol, temperature, or humidity changes or exposure to odors. |
200 | What are the common triggers for vasomotor rhinitis? | Changes in temperature, change in relative humidity, odors (e.g., perfumes, cleaning agents), second-hand tobacco smoke, alcohol, sexual arousal, and emotional changes can be triggers. |
201 | What is the underlying pathophysiology associated with vasomotor rhinitis? | This condition is poorly understood. It may be related to the increased neural efferent input to mucosal vasculature. |
202 | Though controversial, what surgical interventions can be considered in patients with vasomotor rhinitis? | Vidian neurectomy |
203 | What type of nonallergic rhinitis manifests with perennial symptoms including sneezing, watery rhinorrhea, nasal pruritus, and intermittent hyposmia/anosmia; demonstrates ~10 to 20% eosinophils on nasal smear, and is associated with negative in vivo and in vitro allergy testing? | NARES |
204 | A 33-year-old man has profuse watery rhinorrhea whenever he eats his favorite hot and spicy meals. What is the likely diagnosis? | Gustatory rhinitis |
205 | What is the underlying pathophysiology of gustatory rhinitis? | Vagally (cholinergically) mediated vasodilation after eating (especially with hot or spicy foods) |
206 | What type of rhinitis is can be associated with (1) inhaled protein or chemical antigens that result in an IgE-mediated response (allergic rhinitis), (2) inhaled chemical respiratory sensitizers that cause an unknown immune response, or (3) exacerbation of rhinitis and is often associated with concurrent asthma? | Occupational rhinitis |
207 | Pregnancy, puberty, menstruation, and hypothyroidism can all be associated with what type of rhinitis? | Hormonally induced rhinitis |
208 | During pregnancy, hormone-induced vasodilation, vascular pooling, and increased blood volume can contribute to congestion and rhinitis. Is it more common for this to occur as a new diagnosis of rhinitis or as an exacerbation of preexisting rhinitis? | 1/3 of women = exacerbation 2/3 of women = de novo = typically resolves ~2 weeks after delivery |
209 | What are some common medications that can cause rhinitis? | Angiotensin-converting enzyme (ACE) inhibitors, β-blockers and other antihypertensives, erectile dysfunction or pulmonary hypertension medications (i.e., sildenafil), oral contraceptives and aspirin in sensitive individuals. Ethanol in wine, beer, and other alcoholic beverages can result in vasodilation and rhinitis. |
What condition is associated with rebound nasal congestion secondary to using topical nasal decongestants (α-adrenergic) for more than 5 to 7 days? | Rhinitis medicamentosa | |
211 | What condition is associated with degeneration of sinonasal sensory and autonomic nerve fibers leading to mucosal gland involution, squamous metaplasia of the sinonasal epithelium, and significant alteration of mucociliary transport and can be either primary or secondary (after surgery or trauma)? | Atrophic rhinitis (also called rhinitis sicca or ozena) |
212 | What organism commonly colonizes the nasal mucosa in patients suffering from atrophic rhinitis? | Klebsiella ozaenae |
213 | What are the clinical examination findings associated with atrophic rhinitis? | • Foul odor • Yellow/green crusting • Atrophic/fibrotic mucosa |
214 | In addition to the categories of rhinitis included above, what important inflammatory-immune diseases are also associated with nonallergic rhinitis? | • Granulomatous infections (rhinoscleroma, rhinosporidiosis) • Wegener granulomatosis • Sarcoidosis • Midline granuloma • Churg-Strauss syndrome • Relapsing polychondritis • Amyloidosis (Covered in the section on inflammatory/infectious nasal masses and Systemic Disease sections of this chapter) |
215 | What management options have demonstrated utility in the management of nonallergic rhinitis? | • Intranasal glucocorticoids* • Intranasal antihistamine (azelastine [Astelin, Astepro], olapatadine [Patanase])* • Intranasal ipratropium bromide (Atrovent) • Nasal irrigation • Adjunctive oral medications (antihistamines, decongestants) *Primary management: Use full dose daily, often in combination (results are better with intranasal steroid and antihistamine than with either alone). |
216 | What specific feature of nonallergic rhinitis is the target of ipratropium bromide intranasal spray? | Watery rhinorrhea |
217 | What is the proposed reason an intranasal antihistamine nasal spray would offer a benefit to patients with nonallergic rhinitis? | Anti-inflammatory: Decreased eosinophil activation, expression of adhesion molecules, and cytokine production. Potentially decreases neurogenic excitation from olfactory stimuli. |
 Infectious rhinitis
Infectious rhinitis Vasomotor rhinitis (60%)
Vasomotor rhinitis (60%) Nonallergic rhinitis of eosinophilia syndrome (NARES)
Nonallergic rhinitis of eosinophilia syndrome (NARES) Gustatory rhinitis
Gustatory rhinitis Occupational
Occupational Hormonally induced
Hormonally induced Medication induced
Medication induced Atrophic
Atrophic Inflammatory/immune-related disorders
Inflammatory/immune-related disordersAcute and Chronic Rhinosinusitis
218 | In the past decade, the term rhinosinusitis has been commonly used to describe what condition? | Inflammation of the nose and paranasal sinuses. This term is preferred over sinusitis because sinusitis almost always involves the nasal cavity. |
219 | According to the European Position Paper on Rhinosinusitis and Nasal Polyposis (2007), what are the criteria for diagnosing rhinosinusitis? | Inflammation of the paranasal sinuses, with two or more of the following: • Nasal blockage, obstruction, congestion, or nasal discharge (anterior and/or posterior) • ± Facial pain or pressure • ± Hyposmia or anosmia |
Describe the five major classifications of rhinosinusitis based on symptom time course. | • Acute: < 4 weeks with complete resolution • Recurrent Acute: Four or more episodes per year lasting ≥ 7 to 10 days; complete resolution between episodes • Subacute: 4 to 12 weeks; controversial designation (considered as a “filler term”) • Chronic (± NP): > 12 weeks, without complete resolution • Acute exacerbations of CRS: Worsening from baseline chronic symptoms, followed by return to baseline | |
221 | What is one of the tools used to assess the severity of rhinosinusitis symptoms? | • 10-cm visual analog scale: “How troublesome are your symptoms of rhinosinusitis?” • Range: 0 = Not troublesome, 10 = Worst thinkable • 0 to 3 = Mild • 3 to 7 = Moderate • 7 to 10 = Severe |
222 | Define double worsening/sickening. | Symptoms that worsen following initial improvement |
223 | What type of acute rhinosinusitis occurs two to five times per year in the average adult, has a symptom peak at 2 to 3 days, progressively improves after day 5, and has symptom resolution by day 10 to 14? | Acute viral rhinosinusitis |
224 | What are the two most common pathogens associated with acute viral rhinosinusitis? | Rhinovirus and Influenza virus |
225 | What percentage of viral rhinosinusitis is estimated to progress to bacterial sinusitis? | 0.5 to 2% |
226 | What type of acute rhinosinusitis lasts for > 10 days or manifests with worsening of symptoms after day 5? | Acute bacterial rhinosinusitis (ABRS) |
227 | In addition to the diagnostic symptoms associated with rhinosinusitis, what secondary symptoms may suggest ABRS? | Fever, aural fullness, cough, myalgias, or headache |
228 | What pathogens are most commonly involved in ABRS? | • Streptococcus pneumoniae (30%) • Haemophilus influenzae (20 to 30%) • Moraxella catarrhalis (10 to 20%) |
229 | What workup is recommended for acute rhinosinusitis? | • Not recommended: CT or X-ray • CT may be considered for severe disease, immunocompromised patients, clinically suspicious complications, preoperative evaluation, or evaluation of recurrent acute rhinosinusitis. Optional • Anterior rhinoscopy • Nasal endoscopy: Consider for initial workup, if disease is refractory to empiric treatment, for unilateral disease, when symptoms are severe or disabling • Nasal culture: Treatment failure, complications |
230 | When should you consider a sinus puncture using a large-bore needle through the canine fossa or inferior meatus for workup of acute rhinosinusitis? | • Clinical trials: Standard for identifying bacterial pathogens in the maxillary sinuses • Potentially useful if episodes are refractory to treatment or when rapid diagnosis and identification of pathogens are required (e.g., in an immunocompromised patient) |
231 | According to the European Position (EPOS) Paper on Rhinosinusitis and Nasal Polyposis (2007) and supported by data in EPOS 2012, what treatment strategy should be used for mild acute rhinosinusitis with symptoms lasting < 5 days or improving after 5 days? | Symptomatic treatment • Decongestant • Saline irrigation • Analgesics |
Why do some guidelines on acute rhinosinusitis recommend against using mucus color to dictate antibiotic use? | Mucus color is driven by neutrophils, not bacteria. | |
233 | If a patient has moderate to severe symptoms of acute rhinosinusitis that persist or worsen after 5 days, what is the recommended treatment according to the European Position Paper on Rhinosinusitis and Nasal Polyposis (2007) and supported by data in EPOS 2012? | Initiate intranasal corticosteroids. If no improvement is seen after 14 days → reconsider diagnosis, perform nasal endoscopy, consider an intranasal culture, and consider imaging. Also consider antibiotics, if indicated, if no improvement has occurred after 14 days. |
234 | For a patient with acute rhinosinusitis with a temperature > 38°C or in severe pain, what treatment is recommended? | • Intranasal corticosteroids • Antibiotics Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|