Rhinectomy
Fernando Luiz Dias
INTRODUCTION
The nose challenges the oncologic and reconstructive surgeon with special difficulties related to its central location on the face and its complex three-dimensional architecture. The prominent position of the nose accounts for its constant exposure to sunlight and thus for its predisposition to the development of cancer of the skin. The nose is the most common site of involvement of cancer of the skin, and it is also the most common site of recurrence. Rhinectomy is defined as the removal of the vast majority of the nasal framework, soft tissues, and skin. It is a relatively uncommon procedure with most published series including small numbers of patients managed with a three-dimensional nasal resection for cancers of the skin. The multiple factors that make the cancer of the nose an area at increased risk for aggressive behavior and high recurrence include:
Increased actinic exposure
Relative lack of subcutaneous tissue
Enhanced access to perichondrium and periosteum
Close proximity of embryologic fusion planes
Overly conservative treatment (in order to avoid cosmetic deformity)
Complex three-dimensional architecture
Multicentricity of cutaneous malignancy
HISTORY
Nasal swelling and the presence of an external nasal lesion are the most frequent presenting signs or symptoms. An obvious tumor mass, pain, and nasal obstruction are also common. Other symptoms included epistaxis, inflammation, foul odor, purulent discharge, rhinorrhea, headache, nasal septal perforation, epiphora, nasal collapse, threatened loss of vision, and poor fit of dentures.
PHYSICAL EXAMINATION
Although the clinical characteristics of an advanced cancer of the nose are usually obvious under observation, a careful bimanual palpation is advisable in order to evaluate the involvement of the upper lip, columella, and floor of the nasal cavity (Fig. 21.1A). Endoscopic evaluation of the nasal cavity is crucial in accurate clinical assessment of an intranasal lesion. Despite the low incidence of lymph node metastases found in most
published series, even in patients with other histologic types than basal cell carcinoma, a careful palpation of the facial, periparotid, and cervical lymph nodes (particularly levels I and II) is advisable (Fig. 21.1B).
published series, even in patients with other histologic types than basal cell carcinoma, a careful palpation of the facial, periparotid, and cervical lymph nodes (particularly levels I and II) is advisable (Fig. 21.1B).
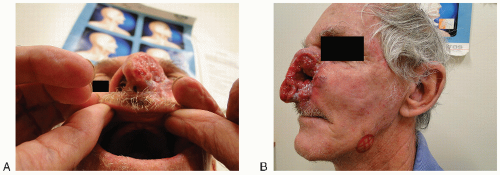 FIGURE 21.1 A: Squamous cell carcinoma of the nose with involvement of the upper lip and gingivobuccal sulcus. B: Lymph node metastases from cutaneous nasal SCC. |
INDICATIONS
The local spread of cancer of the facial skin appears to be markedly influenced by embryologic fusion planes as well as the surrounding facial structures. These fusion planes tend to set up individual areas in which cancer of the skin appears to spread rapidly, invading deeply before continuing its superficial spread that would cross a fusion plane. Soft tissue invasion of these neighboring regions may eventually lead to bone or nerve involvement, making tumor eradication much more difficult.
Five anatomical areas of the midface exist in which there is a rather constant reproducible type of spread of cancer. Cancers located over the supratip and columella tend to invade into the nose along the septum with the later site contributing to invasion of the superior aspect of the midlip and premaxilla. Lesions located along the lateral aspect of the nose tend to spread in a caudal-cephalic manner with through-and-through defects occurring along the nares. Cancers of the skin originating in the nasolabial fold tend to invade deeply toward the pyriform aperture and the nasal cavity before spreading on the cheek and lateral aspect of the upper lip. Cancers located in the glabella and root of the nose are prone to invade deeply and laterally toward the medial canthi. Cancers of the skin of the cheek tend to spread in a uniform nature from their central foci extending into the lower eyelid and upper lip while avoiding nasal involvement.
The columella appears to be a particularly high-risk site; cancers at this site have been described by many authors as a “potential time bomb.” Such tumors may extend directly along the septal cartilage, posteriorly into the nasal cavity, inferiorly into the maxilla, and superiorly into the anterior skull base, meaning that recurrence is often detected late and is extremely difficult to treat. In addition to that, it is the region of the nose most prone to develop lymph node metastases (Fig. 21.2A and B).
The nasal vestibule is studied separately from other sites of the nose, because it is considered part of the nasal cavity. Carcinomas restricted to the nasal cavity are uncommon accounting for only 20% of all cancers arising in the paranasal sinuses and nasal cavity. The nasal vestibule is also considered the subsite in the nasal cavity that is least often affected by cancer, with most cancers arising from the turbinates. Other subsites affected in descending order of frequency are the nasal septum and floor of the nose. Carcinomas of the vestibule are usually of low histologic grade and demonstrate a relatively low metastatic potential. Lymphatic spread, when occurs, does to the facial and parotid lymph nodes first, before they reach levels I and II. Only 40% of the patients with positive nodes ultimately survive.
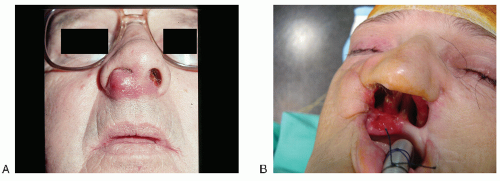 FIGURE 21.2 A: Squamous cell carcinoma of the columella. B: Recurrence of cancer following composite resection of the columella, upper lip, premaxilla, and floor of the nose. |
CONTRAINDICATIONS
There are few contraindications to surgery based on the local factors, all related to the invasion of critical intracranial structures. Although uncommon, these situations are associated with huge invasive/destructive lesions of the midface and share the same contraindications as the resection of skull base tumors. Patients with comorbidities such as severe cardiovascular and/or pulmonary disease, markedly debilitated or demented patients, or those with end-stage renal disease are usually not candidates for surgery.
PREOPERATIVE PLANNING
Imaging Studies
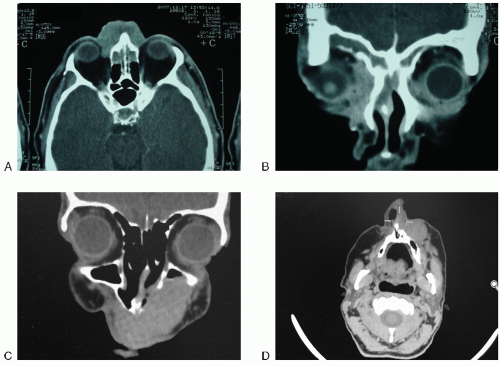
Imaging studies should always be performed as they provide valuable information that can help in the evaluation of tumor extension, particularly the involvement of paranasal sinuses and orbital cavities. Both computed tomography (CT) and magnetic resonance imaging (MRI) are used in the evaluation of large cancers and the surrounding bone structures. Evaluation of periosteal/bone invasion, as well as invasion of nasal and paranasal sinus cavities, is of utmost importance for surgical planning (Fig. 21.3A-D).
Pathology
Due to the bewildering array of malignancies arising on the skin of the face, accurate pathologic diagnosis is critical. If the patient has not been biopsied previously, obviously biopsies must be done. If patients have been biopsied elsewhere, the slides should be reviewed to make certain of the correct diagnosis.
SURGICAL TECHNIQUE
Under general endotracheal anesthesia, the oropharynx is packed with a damp gauze bolster to prevent aspiration. The patient is prepped and draped, with the face, forehead, and neck exposed for those patients who will receive a neck dissection. Ointment is placed in both eyes, and the eyelids are taped or sutured shut. The proposed area of surgical excision is marked with the surgical pen to delineate adequate surgical margins (Fig. 21.4A).
 Get Clinical Tree app for offline access 
|


