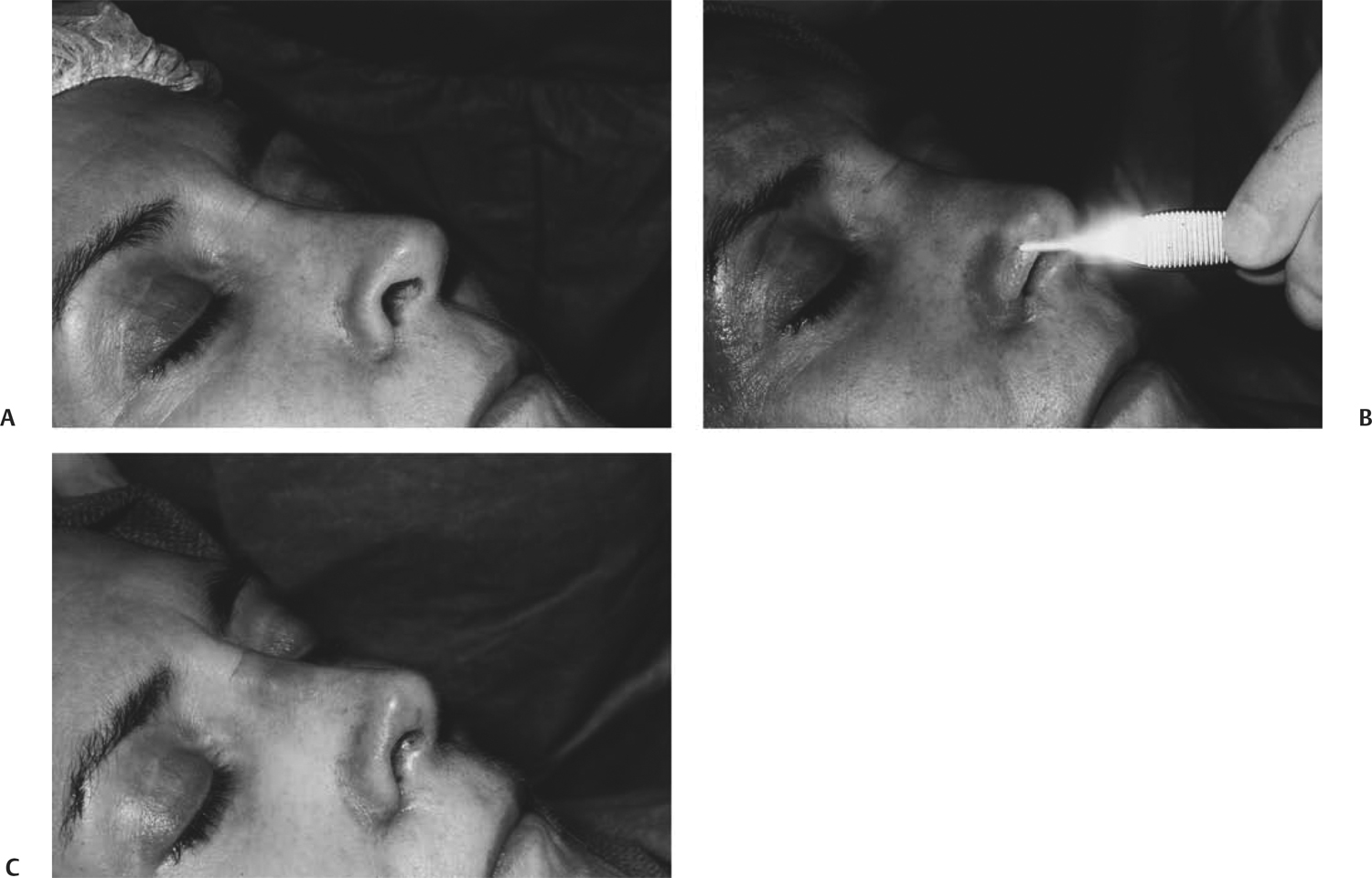
30 Revision Surgery of the Nasal Tip Most aesthetic problems following rhinoplasty involve the lower one third of the nose. The ability to adequately and consistently refine the nasal tip remains the holy grail of the rhinoplasty surgeon. Fortunately, most postrhinoplasty tip problems are minor; some, however, can be daunting. Most postrhinoplasty deformities can be repaired with a fairly reliable degree of aesthetic resolution. It is impossible to assure perfection in any case. The most challenging aspect of revision surgery of the nasal tip may be the surgeon’s ability to balance the patient’s expectations with the reality of what is possible. Postoperative aesthetic problems in the nasal tip result from an inappropriate preoperative evaluation and diagnosis, an inappropriate operative procedure, or both. Each case where the postoperative result is not adequate should represent a valuable learning experience for the surgeon. In each of these less than desirable cases, the preoperative photos should be examined, the operative plan should be reevaluated, and the operative procedure should be reconsidered. Where did the judgmental error occur? This question must be answered. When the surgeon is dealing with his or her own results, the reevaluation provides a humbling but very important enlightening experience in the quest for consistently good results in rhinoplasty. It is much more difficult, though, when the patient has come for secondary surgery with the primary procedure done elsewhere. When a patient who has had a primary rhinoplasty comes to the same surgeon for a secondary procedure, it is usually because the patient has faith in the primary surgeon and trusts that he or she can adequately adjust the aesthetic concerns. It is important that the surgeon acknowledge the problem with which the patient is concerned. It is the beginning point for any reasonable conversation about secondary surgery. There is a strong tendency for the surgeon’s ego to deny that any problem exists. A comment such as “I don’t see any problem” or “It looks fine to me” instantly destroys the patient’s confidence in the surgeon. After all, if the surgeon cannot see the problem, how could he or she fix it? The patient’s next thought would be, “Maybe I shouldn’t have come here in the first place.” It is always best to acknowledge the problem (unless there really is no problem) and deal with it from that point. It is much better to say, “I see what you’re talking about. It’s very minor; I think we should leave it alone.” If the problem, however, is significant, the patient should be told to wait for an appropriate time, and a secondary procedure will be done. If the problem is significant and it is beyond the surgeon’s ability to correct, the case should be referred. When the patient has had surgery elsewhere a long time ago, there is a different set of psychological circumstances. Patients who have had their initial rhinoplasty years ago have usually adjusted to the aesthetic problems, and although they have never been happy with the results, they tend not to be hostile. In many cases financial or family circumstances have had a priority in their life. The initial surgeon may no longer be available. Referring such patients back is not an option. These patients usually are realistic about what can be achieved with secondary surgery. With this group of patients, it is unwise to change their appearance too much, especially relative to overall nasal size and retroussé. Many older patients have the small noses that routinely resulted from operations done in the 1960s and 1970s. They have assimilated the small size into their self-image. The secondary procedure should be designed to bring symmetry and harmony to the nose without significantly enlarging it. These patients will not tell you they do not want the nose larger. Unhappiness about the new, larger nose will be expressed following the secondary procedure. Patients who are seeking secondary rhinoplasty following a recent procedure (1–3 years) represent yet another set of psychological circumstances. Invariably, such a patient has made a decision not to return to the initial surgeon for a secondary procedure. It has been written many times that the primary surgeon should never be admonished about the result. This advice is still true. It accomplishes nothing in helping the patient; Instead, it rekindles any hostility the patient may have. The condemnation of another surgeon always results in some repercussion. It is best to state truthfully that you were not present at the initial surgery and could not possibly know the details of the surgery or the exact reasons that led to the current appearance. You should indicate that you have to examine and evaluate the nose and formulate a plan for secondary rhinoplasty. There are certain patients who are not physically suited for surgery. For example, a patient with exquisitely thin skin may not be suitable for any further manipulation of the tip skin and may not be a candidate for grafting. Conversely, a patient with extremely thick skin may also present a problem for revision surgery. Invariably, such a patient had thick skin when he or she presented to the original surgeon. In an attempt to modify the tip contours, most or all of the lower lateral cartilages (LLCs) were removed, leaving the patient with an even worse looking nose. Most of these patients can be helped by nasal tip grafts, but it is the expectations of these patients that may be a problem. These patients always seem to bring photos of models with small, highly refined noses as their ideal. Surgery should proceed only after the patient truly understands the limitations of revision surgery. Multiple nasal tip procedures in some patients have created a subcutaneous scar tissue density that resists expansion of grafts. Some patients complain more about the dense erythema of the nose following multiple rhinoplasties than about the configuration of the nose. Although newer technologies such as laser and intense pulsed light treatments may be of help, these patients should know that the erythema may worsen. Finally, any medical condition that would preclude other elective procedures would also preclude revision nasal surgery. Most postoperative tip problems result from misjudgments about the preoperative condition of LLCs and a failure to appreciate the significance of thick skin. The most common complaints following rhinoplasty are tip asymmetries (including bossae), poor projection, pollybeak, and tip ptosis. These nasal tip deformities have in common the lack of structural support of the LLCs following surgical intervention. It is almost certain that these patients had LLCs that were relatively nonsupporting before surgery. The second most common complaint is related to alar retraction, alar convexity/concavity, or hanging columella. In the case where tip asymmetries or poor projection has occurred, the surgeon either did not appreciate the relative weakness of the LLCs or did not adapt the rhinoplasty procedure to compensate for the weakness. Where increasing lower lateral strength was imperative, it was instead weakened. In the case of alar retraction, the surgical procedure involved an over-resection of the lateral ala of the LLC or a failure to recognize mild alar retraction preoperatively. The ala retracted superiorly as scar tissue contracted in response to the removed lateral ala cartilage. The hanging columella usually results from over-resection of the ala or a failure to identify a potential for the columella to appear redundant following surgery. Most ala deformities following rhinoplasty are a combined elevation of the alar rim into an arch with a smaller radius preoperatively and a flattening or concavity of the normal alar arch. This deformity is caused by removal of too much of the vertical height of the lateral crus of the LLC. If at least 6 mm of vertical height of cartilage is left at the conclusion of the rhinoplasty, the appearance of the ala usually is adequate. Almost all alar arch elevation is secondary to overexcision of the lower lateral alar cartilage. The alar arch can be restored with either septal or auricular cymba concha cartilage grafting. It can be done as an independent procedure or can be part of a more extensive nasal tip reconstruction. The cartilage graft must be placed at a position that is near the alar margin to cause the desired effect. A cartilage graft placed in the normal anatomical position will not lower the alar margin once scar retraction has occurred. A pocket is created by entering the ala through the original surgical incision. The dissection is carried downward toward the alar margin. The ideal end point is 1 mm above the free margin of the ala. The graft need not extend laterally into the alar base when only the arch of the ala is of concern. The graft size in the 22 × 6 mm range is usually adequate. In most cases the alar skin lining is not deficient, and a composite skin–cartilage graft is not necessary. It is rare for the original surgeon to have removed alar skin lining. Once the scar tissue bed between the skin and the alar lining is dissected, the alar lining adequacy becomes evident. If, preoperatively, the alar margin is noted to be not only elevated but also rolled inward, there may be a possibility that alar skin lining may have to be replaced. The most desirable graft in such circumstances would be a cymba concha cartilage graft lined with attached cymba conchal skin. It is important that the graft be fairly straight or slightly curved. If too much effort is used to make the graft curve so that it mimics the curve of the nasal ala, it will curve even more when it is placed in the alar pocket. This can produce an undesirable flaring of the nostril. The cartilage graft will maintain its position if the pocket is the same size as the graft. The alar skin is closed with 4–0 chromic suture (Figs. 30.1, 30.2). If a composite graft is used, the alar skin is sutured to the composite graft skin with 4–0 chromic sutures. Fig. 30.1 (A) Postoperative rhinoplasty patient with marked elevation of the right alar margin secondary to overexcision of the lower lateral cartilage. (B) Surgical photo indicating the shape and size of the alar batten graft to support the right ala. The graft must be thick enough to be effective, but thin enough so as not cause distortion of the ala. The graft must be placed in a pocket to within 1 mm of the alar margin to effectively lower the rim position. (C) Immediate postoperative showing the effect of the alar batten graft placement. Fig. 30.2 (A) Preoperative frontal view of elevated right alar margin secondary to overexcision of the lower lateral cartilage. (B)
The Elevated Nasal Ala: The Alar Graft

![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


