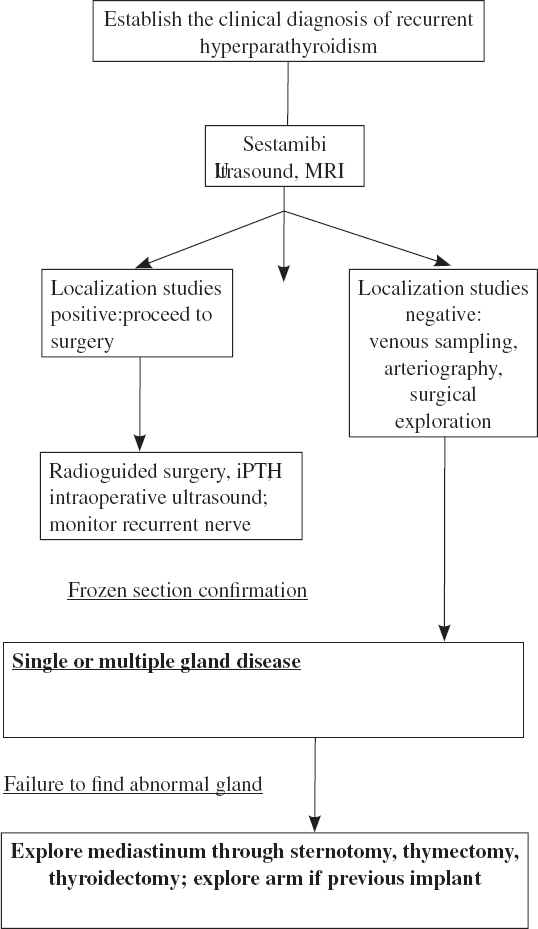
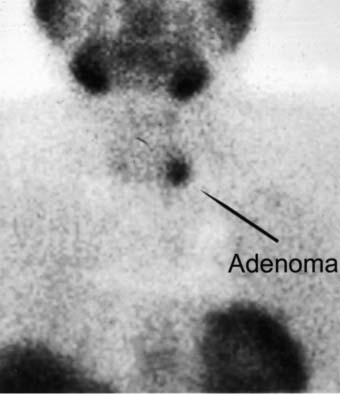
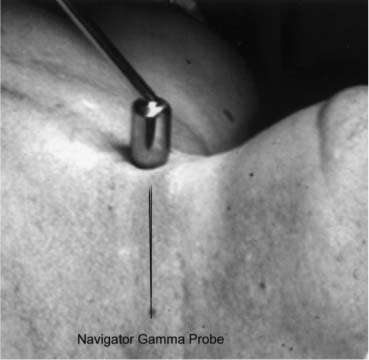
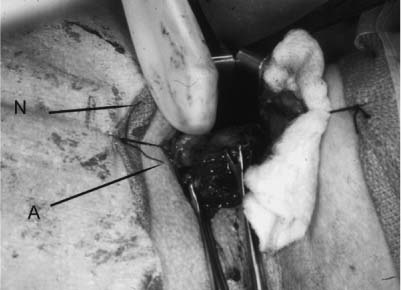
16 Revision Surgery in Parathyroid Disease Revision surgery for hyperparathyroidism can best be summarized by three questions: Is the diagnosis correct? Can the abnormal glands be found? and How can they be removed surgically with minimal morbidity? Whenever a surgeon is referred a patient with suspected recurrence of hyperparathyroidism, the basic principle of making a diagnosis applies. Is this truly a recurrence of hyperparathyroidism, or is this a different disease? Was the original diagnosis correct? What were the patient’s symptoms before the first operation, and have they recurred? Symptoms such as renal colic, abdominal pain, fatigue, and bone pain are commonly seen in parathyroid disease; however, they may also be seen with other syndromes. Signs may include nephrolithiasis, weakness of the proximal muscles of the lower extremities, mental changes, peptic ulcer disease, and chondrocalcinosis in some joints, commonly the knee and pseudogout. Patients can also have nephrolithiasis and hypertension and not have parathyroid disease. Laboratory studies should show elevations of serum calcium, intact parathyroid hormone (PTH), and elevated urinary calcium excretion, the latter requiring the 24-hour creatinine clearance be within the normal range. Supplementary studies may include bone density studies and plain radiographs. Patients with primary PTH may have pain in their long bones, clavicles, hands, and dentition; however, this is more commonly seen with secondary hyperparathyroidism. The physician should inquire if there is any family history or significant endocrine history. Entities that need to be considered include familial hyperparathyroidism, both the autosomal dominant pattern (four-gland hyperplasia) and the recessive (adenoma), and the multiple endocrine neoplasia syndromes, both type 1 (> 90%) and type 2 and their subtypes. One usually sees four-gland hyperplasia in these disease states. Familial hypocalciuric hypercalcemia is another entity that may at times lead the best of clinicians astray. Of paramount importance in diagnosing this disease is the evaluation of renal function and calcium excretion. One of the most important aspects in evaluating the patient is obtaining old records. These should include old operative reports, pathology reports, slides, and old localization studies. Direct communication with the prior surgeon can be invaluable in performing an operation with minimal morbidity. Were any markers left in the patient to identify residual parathyroid tissue, such as a suture or clip? To what were these markers attached? Patients can also be very helpful by their recollection of prior surgery. What were they told after the surgery? How many glands were left? Were the glands in an ectopic location, and were their symptoms and signs improved after surgery? It can be extremely helpful to know if there were any complications after prior surgeries, including hoarseness and hypocalcemia. Did the patient need to take calcium or vitamin D after prior parathyroid exploration? Was the thyroid gland removed as well? How long was the patient symptom free? The diagnostic work-up should rest on the history and physical exam, with confirmation by ancillary studies. Often in parathyroid disease physical signs may be lacking, and the history may be nonspecific. Diagnostic chemistry should include the serum calcium, phosphate, serum protein, thyroid function studies, intact parathyroid hormone (iPTH) level, and urinalysis. A 24-hour urine test for calcium and creatiqnine clearance is mandatory to confirm the diagnosis of hyperparathyroidism and not familial hypocalciuric hypercalcemia (FHH). Hypercalcemia from an occult malignancy should be excluded as well. Radiological testing can include ultrasound, radioisotope studies, computed tomography (CT), magnetic resonance imaging (MRI), and angiography. Selective venous sampling of the arm can help determine the status of implanted glands. Selective internal jugular catheterization for comparative PTH can be helpful in localizing a recurrent lesion (Fig. 16.1). It is understood that the operative procedure must be planned down to the last detail. These patients have had many procedures leading up to this one and, it is hoped, will not have many more. Apart from the localization studies used to help guide the surgical approach, other ancillary procedures, many of which are perioperative, should be thought about and preparations made before the surgery begins. Some of these might include the following: recurrent nerve monitoring, intraoperative PTH assay, gamma probe localization, intraoperative ultrasound, thoracic surgical assistance, arterial access, appropriate permissions, and the ability to store parathyroid tissue long term. Decision tree for revision surgery in parathyroid disease Fig. 16.1 Sestamibi scan showing parathyroid adenoma (2 hours after injection of isotope). Fig. 16.2 Gamma probe applied to neck before incision is made (90 minutes after injection of isotope). Fig. 16.3 Gamma probe used during operative procedure. A, adenoma; N, navigator.
Patient Evaluation
Is the Diagnosis Correct?
What Was Done Previously?
What Needs to Be Done Now?
Planning the Operation
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Ento Key
Fastest Otolaryngology & Ophthalmology Insight Engine
