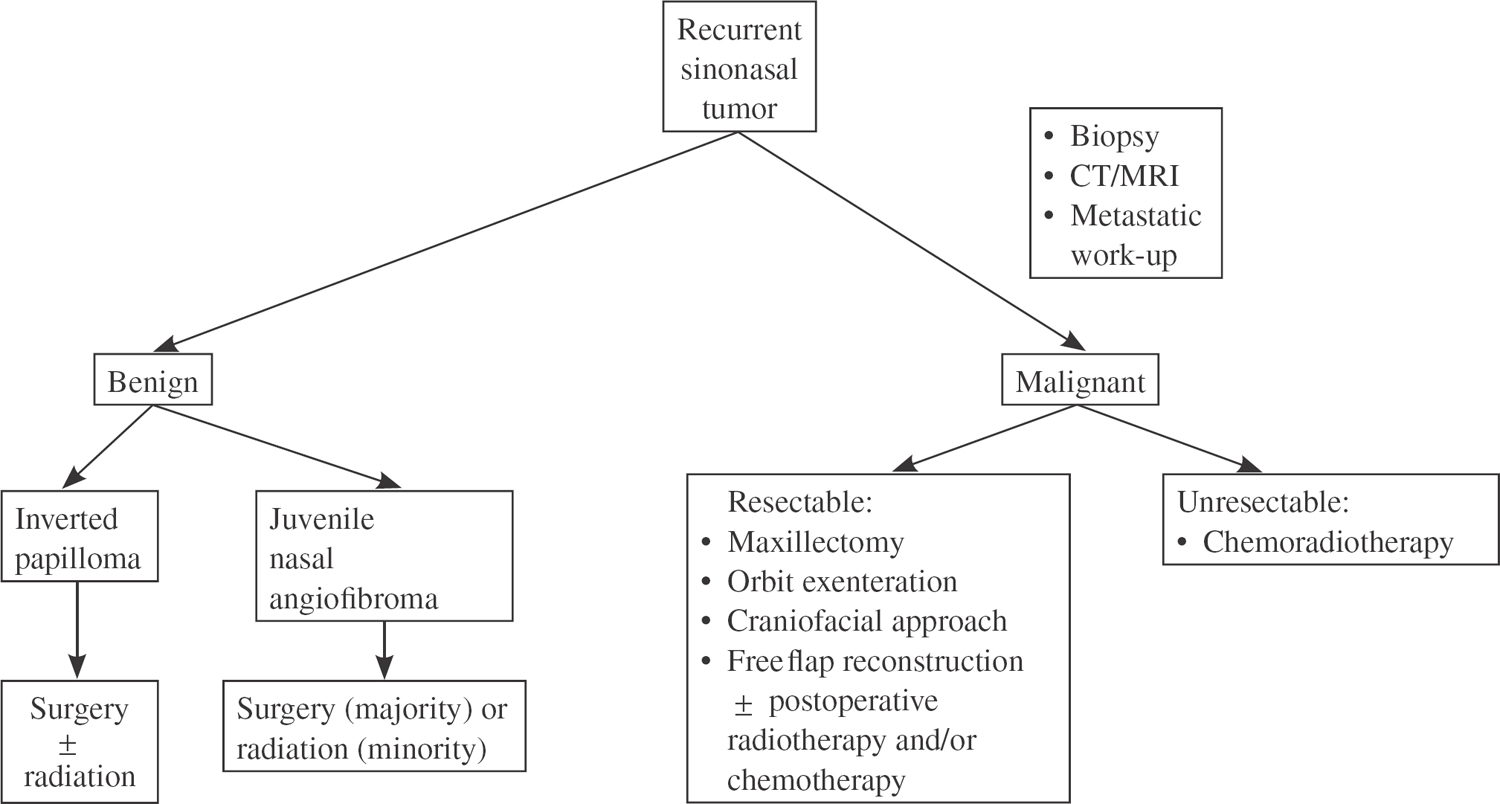
21 Revision Surgery for Paranasal Sinus Tumors Cancer of the paranasal sinus remains a difficult and challenging problem, despite attempts to improve survival and quality of life over the last 2 decades. The prognosis for patients with squamous cell carcinoma of the paranasal sinus remains poor even with advancements in surgical, radiotherapeutic, and chemotherapeutic techniques. Paranasal sinus cancer is uncommon and represents only 0.2 to 0.8% of all malignancies. Cancer of the paranasal sinus constitutes 3% of all carcinomas of the upper aerodigestive tract.1 The majority of paranasal sinus malignancies, 50 to 80%, originate within the maxillary sinus antrum. Malignancies rarely occur within the other sinuses, and originate in the ethmoid, frontal, and sphenoid sinuses in 10%, 1%, and 1%, respectively.2 The cause of paranasal sinus malignancies is unknown. However, several risk factors have been associated with neoplasms of the paranasal sinus. Exposures to radium, chromium, nickel, wood, and leather have been associated with higher incidence of paranasal sinus malignancies.3 The carcinogenic potential of tobacco, alcohol, and viruses has not been directly linked to squamous cell carcinoma of the paranasal sinus. The destructive and devastating nature of squamous cell carcinoma of the paranasal sinus is manifested in the low overall survival rates and high local recurrence rates seen in these patients. Although the ideal curative treatment of paranasal sinus malignancies is dependent upon early diagnosis and controlling the primary tumor site, there is a limited role for salvage surgical intervention for recurrent, persistent, or progressive disease. The indications for revision surgical intervention for recurrent paranasal sinus malignancies will be reviewed. The diagnosis of paranasal sinus malignancies requires a thorough history and physical examination of the head and neck region. The priorities of any clinician who encounters a paranasal sinus neoplasm must include establishing a histologic diagnosis, determining the anatomical extent of the neoplasm, and planning an effective treatment strategy. Typically, the signs and symptoms of early-stage paranasal sinus neoplasm are nonspecific. Initial symptoms may mimic benign paranasal sinus and nasal disorders, including nasal stuffiness, facial pain, headaches, and intermittent epistaxis.4 The natural air-filled cavities of the paranasal sinuses allows for significant growth of the malignancy prior to producing signs and symptoms of local extension.5 The expanding paranasal sinus neoplasm may produce sign and symptoms related to the orbit, brain, nasal cavity, oral cavity, facial soft tissues, and cranial nerves.1,3 Radiologic imaging provides extremely valuable information regarding the location, size, extent, and invasiveness of the paranasal sinus cancer. The imaging studies are invaluable in determining a preoperative treatment plan because they allow the surgeon to better appreciate the extent of the disease and the involvement of important structures. Although there are several imaging techniques available to the surgeon, computed tomography (CT) and magnetic resonance imaging (MRI) have been the most effective modalities for evaluating paranasal sinus cancer. Evaluating a paranasal sinus neoplasm requires a CT scan with intravenous contrast in both the coronal and axial planes. The CT scan provides information regarding the bony architecture of the orbital apex, infratemporal fossa, pterygoids, cribriform plate, and sphenoid and ethmoid sinuses.3,4 When evaluating the paranasal sinus for recurrent, persistent, or progressive cancer, the information from the MRI is additive to the CT scan and provides critical information regarding the soft tissue detail of this complex anatomical region. Involvement of the infratemporal fossa, pterygopalatine fossa, periorbital tissues, peripheral nerves, brain parenchyma, carotid artery, cavernous sinus, and prevertebral fascia can be delineated with MRI scans.3,4 The MRI provides the additional advantages of being able to distinguish tumor from retained secretions and offering image structures in multiple planes. Obtaining the histologic diagnosis of the neoplasm is paramount to determining the treatment plan and prognosis for the patient. The majority of tumors are approachable for biopsy via the endonasal route. If, however, the tumor is contained within the maxillary sinus cavity without extension into the nasal cavity, antrostomy of the sinus may be performed. Either an inferior meatus antrostomy or a Caldwell-Luc approach may be used. It is important to obtain an adequate amount of tissue for histological, immunohistochemical, and electron microscopic analysis.3,6 Decision tree for recurrent sinonasal tumors Paranasal sinus malignancies continue to present therapeutic challenges to the head and neck surgeon. The fact remains that the majority of these malignancies are diagnosed as locally advanced disease because of the vague and nonspecific nature of symptoms in early-stage lesions. Several studies report a preponderance of patients presenting with T3 or T4 lesions.2,4,5,7,8 The primary treatment strategies of various institutions has consisted of surgery, radiation therapy, or combination therapy.4,6 Although considerable experience have accumulated in the treatment of paranasal sinus cancer with primary radiation therapy, only combined modality and revision surgical therapy will be discussed.5,8 Advanced lesions of the paranasal sinuses traditionally have been treated with combination therapy consisting of either pre- or postoperative radiation therapy and surgery. The surgical procedures consist of either partial maxillectomy, total maxillectomy, radical maxillectomy, or cranial base surgery.4,9–11 The descriptions of the surgical techniques are beyond the scope of this chapter and are well described elsewhere. Surgery of recurrent, persistent, or progressive paranasal sinus cancers is designed to achieve the highest possible cure rates with the least anatomical and functional deformities.4 Revision surgery is often limited to cryotherapy or laser debulking, because the primary surgical treatment usually consists of a total maxillectomy, radical maxillectomy, or cranial base surgery of a locally advanced paranasal sinus cancer.1,4,11 The extent of revision surgery is predicated upon the respectability of the lesion. The extension of the primary, recurrent, or progressive paranasal sinus cancer into a substantial portion of the brain parenchyma, bilateral cavernous sinuses, or both optic nerves may preclude the lesion from being surgically resectable.3,4 However, in selected cases of extensive disease, revision surgical treatment may offer the most effective form of palliation.3,4,11 The debate over whether radiation therapy should be given before or after surgery continues. The proponents of preoperative radiation therapy advocate giving radiation first because the blood supply to the tumor has not been altered; hence the tumor tissue is better oxygenated. Additionally, it may be more likely to achieve clear surgical margins because preoperative radiation has its greatest impact on the periphery of the tumor.9,12 The proponents of postoperative radiation therapy maintain that radiation therapy is most effective when the tumor burden is small. Also, postoperative radiation therapy allows for more accurate assessment of the extent of disease and reduces concern with surgical wound healing, allowing for the administration of a higher total dose of radiation.13 Advances in the planning and delivery techniques of radiation therapy have allowed for innovative protocols for treating recurrent or persistent paranasal sinus malignancies. Further advances in intensity modulated radiation therapy (IMRT), three-dimensional conformal therapy, brachytherapy, and altered fractionation of radiation therapy have allowed for re-irradiation protocols for recurrent paranasal sinus cancers.14 IMRT allows precise delivery of radiation beams, thus reducing associated morbidity. Although the follow-up period has been short, several studies have shown that radiation treatment with IMRT for paranasal sinus cancers is associated with lower rates of dry eye syndromes and other visual disturbances.13,14 Chemotherapy has several roles in the treatment of recurrent paranasal sinus cancers. As an induction agent, it may cause tumor shrinkage. In combination with radiation, it may act as a radiosensitizing agent for recurrent or metastatic disease. However, chemotherapy in several protocols has not increased survival rates.12,15 The higher incidence of paranasal sinus cancer in Japan has encouraged investigators there to develop alternative combined therapy. The combined treatment modality used by several institutions in Japan consists of simultaneous radiation therapy, intra-arterial chemotherapy, and conservative surgery.16
Diagnosis
Treatment
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Revision Surgery for Paranasal Sinus Tumors
